






Health reform will insure roughly 30 million Americans who would otherwise go uncovered. Roughly half will be covered through Medicaid. This angers conservatives, who argue that Medicaid costs too much, that it overly burdens the states, and that Medicaid even harms its own recipients. The word “welfare” pops up conspicuously often, too. Conservative health policy commentator Avik Roy writes the appalling sentence:
Health reform critics provide scary projections by lumping together Medicare, Medicaid, and Social Security. Only the first – Medicare – is on a truly frightening path.
“It’s Medicaid, i.e., welfare dependency, that leads to family breakdown and social disrepair.”
Rep. Paul Ryan similarly calls the House Republican budget “welfare reform round two,” adding:
“[W]e don’t want to turn the safety net into a hammock that lulls able-bodied people to lives of dependency and complacency, that drains them of their will and their incentive to make the most of their lives.”
Meanwhile, Mitt Romney proposes not only to repeal health reform, but to turn Medicaid into a block grant arrangement worse than we had before. Under a block grant, the federal government would give each state a fixed amount every year. Over time, block grants would grow more slowly than the true cost of care, shifting huge costs and risks onto states and, ultimately, individual patients. Block grants provide huge incentives for states to drop services such as dental care and to restrict eligibility.
Medicaid problems only worsen with cuts
Medicaid could operate better. For example, it notoriously underpays doctors and hospital, many of whom respond by shunning Medicaid recipients. Such problems arise because Medicaid is under-funded, and because it relies too much on states that lack the money and governing capacity to bear this load. Basic values matter, too. Many states have already enacted punishing Medicaid cuts in the current recession. South Carolina’s effort to cut hospice, respite, and meals-on-wheels services are two depressing examples. Cutting federal funding and federal oversight only worsens such problems.
“Repeal and replace” efforts to kill health reform especially focus on repealing the Medicaid expansion that would extend coverage in 2014 to millions of low-income adults and kids. Ironically, these measures are unlikely to much improve the federal budget.
Despite rhetoric of “entitlement crisis,” Medicaid’ spending growth will be quite manageable, particularly at the federal level. Health reform critics provide scary projections by lumping together Medicare, Medicaid, and Social Security. Only the first – Medicare – is on a truly frightening path.
Medicaid’s financial challenges do not arise from millions of basically healthy low-income adults and kids newly covered under health reform. Although these low-income populations account for the majority of Medicaid recipients, this group now accounts for only about one-third of actual Medicaid spending.
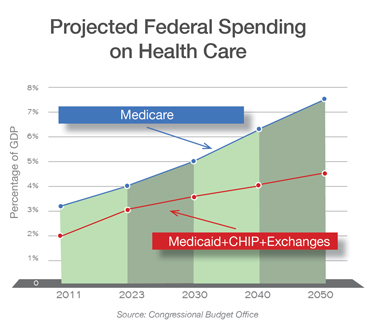
The Congressional Budget Office is as close to an official budget scorekeeper as we are likely to have in public policy. Last month, CBO released updated projections for federal spending to 2050. The graph above plots these results as a percentage of our economy, as indicated by the gross domestic product (GDP). The blue line indicates Medicare spending. The flatter red line indicates combined federal spending on Medicaid, the new health insurance exchanges, and the Children’s Health Insurance Program.
Health reform causes an initial spending bump for new coverage. Over time, though costs are projected to rise more slowly in Medicaid than among either Medicare recipients or the privately insured. By 2050, the federal government is projected to spend 60 percent more on Medicare than it will on Medicaid, CHIP, and the new health insurance exchanges. I fear the federal government will spend too little on Medicaid, since states have such difficulty carrying their share of the load.
Program’s financial challenges aren’t due to health reform
To the extent that Medicaid does present financial challenges, these do not arise from millions of basically healthy low-income adults and kids newly covered under health reform. Although these low-income populations account for the majority of Medicaid recipients, this group now accounts for only about one-third of actual Medicaid spending.
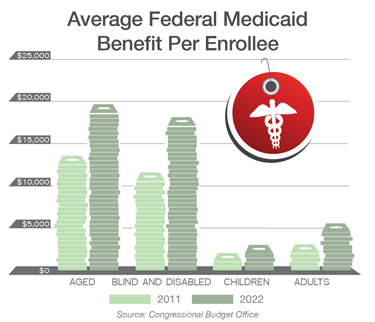
As shown in the second graph, the federal government spends five times as much on every aged, blind, or disabled recipient as it does on the average non-disabled working-age adult. Children are even cheaper. My colleague Aaron Carroll notes that one must deprive literally millions of able-bodied low-income people of coverage to have a large financial effect. Although the aged and disabled are where the real money is, it’s complicated and politically risky to reduce spending on these visibly sympathetic and often-organized groups. It’s much easier to roll back promised coverage for the typically uninsured person helped under health reform. That’s exactly what I therefore expect Republicans to do.
Opponents feel some urgency in killing the Medicaid provisions of health reform. Their main urgency is political. These provisions will be hard to repeal once individuals and state governments become accustomed to them. As former Bush administration official James Capretta told me last year, “As soon as the money starts flowing, you can’t stop it.”
I hope so.