Find Kansas Health Insurance Marketplace Coverage for 2026

Compare ACA plans and check subsidy savings from a licensed third-party health insurance agency.
Kansas Health Insurance Marketplace Guide
Use this guide, including the FAQs below, to help you find the right health plan in Kansas. Many people find an ACA Marketplace plan, also known as Obamacare or exchange, to be a cost-effective choice.
Kansas uses the federally-facilitated health insurance Marketplace, which is HealthCare.gov. The HealthCare.gov platform allows Kansas residents to select from among a variety of health plans, and receive income-based financial assistance if eligible.
For 2026, six private insurers offer individual/family health plans through the Kansas exchange,1 down from seven in 2025. And at least one more insurer is exiting the Kansas Marketplace at the end of 2026 (see details below about insurer participation for 2027).
*Values displayed by this tool are from data generated by CMS and reflect 2026 Marketplace health plans purchased in each state. The values returned are averages based on the plans purchased by consumers of each selected state: subsidy and premium values vary based on factors such as zip code, age, household size, and income.
Kansas Marketplace quick facts
Frequently asked questions about health insurance in Kansas
Who can buy Marketplace health insurance in Kansas?
You must meet certain criteria to qualify for health coverage through the Marketplace in Kansas. Generally, you’re eligible to apply if you:4
- Live in Kansas and are lawfully present in the U.S.
- Are not incarcerated
- Are not enrolled in Medicare
By those standards, most Kansas residents can use the Marketplace. But eligibility for financial assistance is also an important factor. To be eligible for income-based subsidies, you must:
When can I enroll in an ACA-compliant plan in Kansas?
Open enrollment for 2026 individual/family health insurance ended January 15, 2026 in Kansas.
Outside of open enrollment, you can get coverage through the Marketplace if you have a qualifying life event that triggers a special enrollment period (SEP).
Examples of qualifying life events include loss of health coverage, getting married, or permanent relocation (marriage and a permanent move will only trigger a special enrollment period if you already had coverage in place before the life event; for marriage, at least one spouse must have already had coverage). Learn more about special enrollment periods.
Note: American Indians and Alaska Natives can enroll in an ACA exchange plan year-round.
The open enrollment period for 2027 coverage might end on December 15. But in June 2026, a judge vacated the federal rule change that had mandated the shorter open enrollment period.7
HHS could appeal the ruling, or might just continue to use the open enrollment schedule that was used for the past several years, with a January 15 end date. Kansas Marketplace enrollees should pay close attention to any communications they receive regarding deadlines for 2027 coverage.
Where do I enroll in a Marketplace plan in Kansas?
If you’re eligible for an ACA Marketplace plan, there are a few ways to enroll, with or without free assistance:
- Online through HealthCare.gov
- By phone at (800) 318-2596
- With the help of an agent/broker, navigator, or certified application counselor (help is available online, over the phone, or in person)
- Via an approved enhanced direct enrollment entity.8
How can I find affordable health insurance in Kansas?
In Kansas, you can find affordable individual and family health insurance through HealthCare.gov – the ACA Marketplace.
Of the roughly 200,000 people who enrolled in coverage through the Kansas Marketplace for 2026, 89% were eligible for premium subsidies (advance premium tax credits, or APTC) that averaged $697/month. After the subsidies were applied, the average subsidy-eligible Kansas Marketplace enrollee was paying about $80/month for their coverage.9
(Note that for 2026, premium subsidies are still available to most enrollees, but are no longer available to those with household income above 400% of the federal poverty level. In addition, subsidies don’t cover as much of enrollees’ premiums as they covered in 2025. This is because Congress didn’t extend the subsidy enhancements that expired at the end of 2025.)
In addition to APTC, if you’re not eligible for Medicaid/CHIP and your household income is between 100% and 250% of the federal poverty level,10 you will also be eligible for cost-sharing reductions (CSR), as long as you select a Silver-level plan in the Marketplace. CSRs help reduce deductibles and out-of-pocket expenses.
Source: CMS.gov9
You may also find affordable coverage through Medicaid (KanCare) if you’re eligible.
Kansas has not yet implemented the ACA’s expansion of Medicaid for low-income adults. However, children may be eligible for Medicaid or CHIP even if their parents aren’t. For certain families, enrolling children in Medicaid or CHIP while parents get coverage through the Marketplace can be an affordable way to obtain family coverage.
Kansas had been considering changes to its essential health benefits (EHB) benchmark plan starting with the 2025 plan year (recommendations included coverage of hearing aids, bariatric surgery, and applied behavior analysis for autism).11 But appropriations legislation enacted in 202312 prohibited the state from using any funds to make changes to the EHB benchmark plan. As a result, the state halted the process of changing its EHB benchmark plan.13
How many insurers offer Marketplace coverage in Kansas?
For 2026, six insurers offer plans through the Kansas health insurance Marketplace:1
- Ambetter from Sunflower Health Plan/Celtic
- Blue Cross and Blue Shield of Kansas City
- Blue Cross and Blue Shield of Kansas
- Medica Insurance Company (plans terminate at the end of 2026)
- Oscar Insurance Company
- UnitedHealthcare
Medica will no longer offer individual market plans in Kansas after the end of 2026. About 600 Medica enrollees in the Kansas City area will need to select new coverage during the open enrollment period for 2027.14
Learn more: What you need to know when your insurer is leaving the market.
Kansas had seven Marketplace insurers in 2025, but Aetna left at the end of 2025. Aetna exited the individual market in all states where it offered that coverage.
Are Marketplace health insurance premiums increasing in Kansas?
For 2026, the following average rate changes were approved for the insurers that offer coverage in the Kansas Marketplace,15 amounting to a weighted average increase of 26.6%, before subsidies are applied:16
Kansas’ ACA Marketplace Plan 2026 APPROVED Rate Increases by Insurance Company |
|
|---|---|
| Issuer | Percent Increase |
| Ambetter from Sunflower Health Plan/Celtic | 33.7% |
| Blue Cross and Blue Shield of Kansas City | -6.1% |
| Blue Cross and Blue Shield of Kansas, Inc. | 16.7% |
| Medica Insurance Company | 30.8% |
| Oscar Insurance Company | 14.4% |
| UnitedHealthcare | 11.7% |
| Aetna | Exited the market |
Source: Federal Rate Review Summary17
Rate changes apply to full-price premiums. Since most people using the Kansas exchange receive premium tax credits, they don’t pay the full premium amount.18 If you qualify for subsidies, your actual rate change will depend on how your plan’s premium changes, but also how your subsidy amount changes.
For 2026, subsidies don’t cover as much of enrollees’ total premiums and are available to fewer people, because Congress did not extend the federal subsidy enhancements that had been in effect since 2021. The expiration of those subsidy enhancements at the end of 2025, resulted in substantial increases in the amount that people have to pay for their Marketplace coverage.
For perspective, here’s a summary of how overall average premiums have changed over the years for the individual/family market in Kansas, before any subsidies were applied:
- 2015: Average increase of 4%19
- 2016: Average increase of 23%20 (carrier with largest rate increase ultimately left the market)
- 2017: Average increase of 36.6%21
- 2018: Average increase of 29%22 (BCBSKS rate change wasn’t counted because their plans (HMOs) were terminated and replaced with EPOs)
- 2019: Average increase of 5.3%23
- 2020: Average increase of 0.3%24
- 2021: Average increase of 7.8%25 (unweighted average)
- 2022: Average increase of 6%26 (unweighted average)
- 2023: Average increase of 7.2%27
- 2024: Average increase of 7.3%28
- 2025: Average increase of 8.9%29
How many people are insured through Kansas’ Marketplace?
During the open enrollment period for 2026 coverage, 192,811 people signed up for private plans through the Kansas Marketplace.9 This was a decrease from 2025’s record-high enrollment, but was still the highest enrollment had been in any year other than 2025.
The enrollment increase over the last few years (see graph below) was due in large part to the American Rescue Plan (ARP). Under the ARP, the ACA’s premium subsidies were larger and more widely available, and this was extended through 2025 by the Inflation Reduction Act.30
But as noted above, the subsidy enhancements expired at the end of 2025, after Congress failed to extend them. As a result, enrollment declined in 2026 in nearly every state, including Kansas.9
The enrollment growth in 2024 and 2025 was also partially due to the Medicaid disenrollments that resumed in 2023, after being paused for three years during the pandemic. CMS reported that more than 31,000 Kansas residents transitioned from Medicaid to Marketplace coverage during the Medicaid continuous coverage “unwinding” period that began in the spring of 2023.31
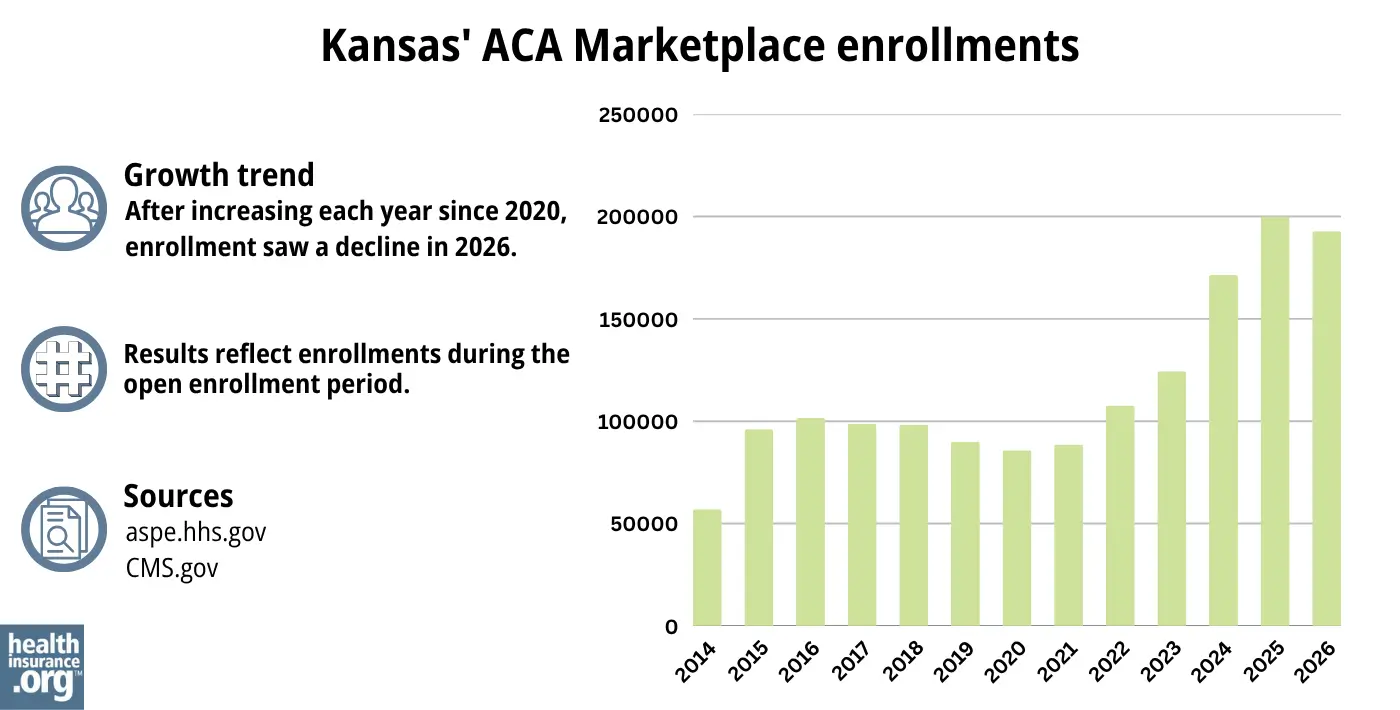
Source: 2014,32 2015,33 2016,34 2017,35 2018,36 2019,37 2020,38 2021,39 2022,40 2023,41 2024,42 202543 20269
What health insurance resources are available to Kansas residents?
Healthcare.gov: This is the ACA Marketplace where you can enroll in a health insurance plan online. You may also get help by calling (800) 318-2596.
Kansas Insurance Department: Call the Consumer Assistance Hotline at (800) 432-2484 in Kansas or (785) 296-7829 if out of state.
Senior Health Insurance Counseling for Kansas (SHICK): SHICK offers help with questions about Medicare.
Medicaid (KanCare): Though Kansas has not expanded Medicaid, certain people who meet the income limits may qualify.

Looking for more information about other options in your state?
Need help navigating health insurance options in Kansas?
Explore more resources for options in KS including short-term health insurance, dental, Medicaid and Medicare.
Speak to a sales agent at a licensed insurance agency.
Footnotes
- ”Kansas Rate Review Submissions” RateReview.HealthCare.gov. Accessed Sep. 18, 2025 ⤶ ⤶
- ”2026 OEP State-Level Public Use File (ZIP)” Centers for Medicare & Medicaid Services, Accessed July 9, 2026 ⤶ ⤶
- ”Kansas Rate Review Submissions” RateReview.HealthCare.gov. Accessed Sep. 18, 2025 *The above is based on the most current data available. ⤶
- “A quick guide to the Health Insurance Marketplace” HealthCare.gov ⤶
- Medicare and the Marketplace, Master FAQ. Centers for Medicare and Medicaid Services. Accessed Jan. 23, 2026 ⤶
- Premium Tax Credit — The Basics. Internal Revenue Service. Accessed Jan. 23, 2026 ⤶ ⤶
- ”City of Columbus et al. v. Kennedy et al. (Columbus I)” O’Neill Institute, Health Care Litigation Tracker. Shorter OEP vacated June 12, 2026 ⤶
- “Entities Approved to Use Enhanced Direct Enrollment” CMS.gov, Apr. 7, 2026 ⤶
- ”2026 Marketplace Open Enrollment Period Public Use Files” CMS.gov. April 2026 ⤶ ⤶ ⤶ ⤶ ⤶
- “Federal Poverty Level (FPL)” Healthcare.gov. Accessed Jan. 23, 2026 ⤶
- ”Kansas Essential Health Benefits Update, Plan Year 2025” Lewis & Ellis Actuaries and Consultants. Oct 13, 2022 ⤶
- ”Kansas Senate Bill 25” BillTrack50. Enacted April 28, 2023 ⤶
- ”ACA – Benchmark Health Insurance Plan Selection” Kansas Insurance Department. Accessed July 2026 ⤶
- ”Medica to exit ACA market in 3 states” Becker’s Payer Issues. June 30, 2026 ⤶
- ”Kansas Rate Review Submissions” RateReview.HealthCare.gov. Accessed Dec. 18, 2025 ⤶
- ”2026 Final Gross Rate Changes – Kansas: 26.6%; ~206,000 Kansans facing MASSIVE rate hikes starting in January (updated)” ACA Signups. Oct. 31, 2025 ⤶
- Kansas Rate Review Submissions. RateReview.HealthCare.gov. Accessed Dec. 18, 2025 ⤶
- ”Effectuated Enrollment: Early 2024 Snapshot and Full Year 2023 Average” CMS.gov, July 2, 2024 ⤶
- Analysis Finds No Nationwide Increase in Health Insurance Marketplace Premiums. The Commonwealth Fund. December 2014. ⤶
- FINAL PROJECTION: 2016 Weighted Avg. Rate Increases: 12-13% Nationally* ACA Signups. October 2015. ⤶
- Avg. UNSUBSIDIZED Indy Mkt Rate Hikes: 25% (49 States + DC). ACA Signups. October 2016. ⤶
- 2018 Rate Hikes. ACA Signups. October 2017. ⤶
- 2019 Rate Hikes. ACA Signups. October 2018. ⤶
- 2020 Rate Changes. ACA Signups. October 2019. ⤶
- 2021 Rate Changes. ACA Signups. October 2020. ⤶
- 2022 Rate Changes. ACA Signups. October 2021. ⤶
- UPDATED: FINAL Unsubsidized 2023 Premiums: +6.2% Across All 50 States +DC. ACA Signups. Accessed November 2023. ⤶
- So How’d I Do On My 2024 Avg. Rate Change Project? Not Bad At All! ACA Signups. December 2023. ⤶
- ”Kansas: Preliminary avg. unsubsidized 2025 #ACA rate changes: +8.9% (semi-weighted); US Health dropping out?” ACA Signups. Sep. 3, 2025 ⤶
- “Health Insurance Marketplaces 2023 Open Enrollment Report”CMS.gov, 2023 ⤶
- HealthCare.gov Marketplace Medicaid Unwinding Report. Centers for Medicare and Medicaid Services. Data April 2024; Accessed Aug. 20, 2024 ⤶
- “ASPE Issue Brief (2014)” ASPE, 2015 ⤶
- “Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report”, HHS.gov, 2015 ⤶
- “HEALTH INSURANCE MARKETPLACES 2016 OPEN ENROLLMENT PERIOD: FINAL ENROLLMENT REPORT” HHS.gov, 2016 ⤶
- “2017 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2017 ⤶
- “2018 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2018 ⤶
- “2019 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2019 ⤶
- “2020 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2020 ⤶
- “2021 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2021 ⤶
- “2022 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2022 ⤶
- “Health Insurance Marketplaces 2023 Open Enrollment Report” CMS.gov, 2023 ⤶
- ”HEALTH INSURANCE MARKETPLACES 2024 OPEN ENROLLMENT REPORT” CMS.gov, 2024 ⤶
- “2025 Marketplace Open Enrollment Period Public Use Files” CMS.gov, May 2025 ⤶

