Find West Virginia Health Insurance Marketplace Coverage for 2026

Compare ACA plans and check subsidy savings from a licensed third-party health insurance agency.
West Virginia Marketplace quick facts
West Virginia health insurance Marketplace guide
West Virginia uses the federally run HealthCare.gov health insurance Marketplace. You can use the West Virginia Health Insurance Marketplace to enroll in health coverage for yourself or your family. The Marketplace also allows you to see if you qualify for premium subsidies or cost-sharing reductions (CSR) to lower your premiums and out-of-pocket costs. The Marketplace is a good option for:
- Self-employed individuals
- Early retirees not yet on Medicare
- People whose employers don’t provide health insurance coverage
Two private insurance companies offer Marketplace plans in West Virginia for 2026,4 both of which also offered coverage statewide in 2025.5 However, CareSource is exiting the individual market in West Virginia at the end of 2026, leaving only one insurer that will offer plans for 2027 (see details below about premium changes for 2026 and carrier changes for 2027).
This guide, including the FAQs below, explains the West Virginia ACA Marketplace and helps you understand your options.
Frequently asked questions about health insurance in West Virginia
Who can buy Marketplace health insurance in West Virginia?
Anyone who meets the following criteria can buy Marketplace health coverage in West Virginia:
- You live in West Virginia
- You’re a U.S. citizen, national, or lawfully present
- You’re not incarcerated
- You don’t already have Medicare
Your eligibility for financial assistance (premium subsidies and cost-sharing reductions) depends on your income. In addition, to qualify for financial help on the Marketplace, you must:
- Not have access to affordable health coverage through your employer. If you think your employer’s health coverage is too expensive, use our Employer Health Plan Affordability Calculator to see if Marketplace premium subsidies are available to you.
- Not be eligible for West Virginia Medicaid or CHIP.
- Not be eligible for premium-free Medicare Part A.6
- If married, file a joint tax return.7
- Not be able to be claimed by someone else as a tax dependent.7
When can I enroll in an ACA-compliant plan in West Virginia?
The next open enrollment period, for coverage effective in 2027, will begin November 1, 2026 and will end on December 15, 2026. This is a shorter window than the one that was used for the last several years, due to a federal rule change. And all plans selected during open enrollment will take effect January 1.
Open enrollment for 2026 health coverage ended on January 15, 2026 in West Virginia.8
To enroll in 2026 coverage (or switch to a different plan) after January 15, 2026, a special enrollment period (SEP) is necessary. In most cases, SEPs are triggered by a qualifying life event. But Native Americans can enroll anytime throughout the year.
How do I enroll in a Marketplace plan in West Virginia?
Use one of the following options to enroll in a Marketplace plan in West Virginia:
- Visit HealthCare.gov
- Call 1-800-318-2596 (TTY: 1-855-889-4325). The call center is available 24 hours a day, seven days a week, except for holidays.
You can find local help from local insurance agents, brokers, or certified application counselors. They help you review Marketplace plan options and choose a plan to fit your needs. Find help at localhelp.HealthCare.gov.9
You can also enroll in a West Virginia Marketplace plan via an approved enhanced direct enrollment entity.10
How can I find affordable health insurance in West Virginia?
You can find affordable health plans in West Virginia on the ACA Marketplace (HealthCare.gov).
Across people who enrolled in West Virginia Marketplace coverage during the open enrollment period for 2026 coverage:11
- 89% of enrollees were receiving advance premium tax credits (premium subsidies).
- The average premium subsidy amount was $1,244 per month (this is the largest average premium subsidy in the nation, because West Virginia has the nation’s highest full-price premiums). After the subsidies were applied, the average net premium for subsidy-eligible West Virginia Marketplace enrollees was about $80/month.
- Thirty-nine percent of West Virginia Marketplace enrollees signed up for plans with built-in cost-sharing reductions (CSR), which are available on Silver-level plans if household income isn’t more than 250% of the federal poverty level.12 CSRs help reduce deductibles and other out-of-pocket expenses.
West Virginia has the nation’s highest average Marketplace premiums,11 which makes premium subsidies particularly important for ensuring affordability.
But because Congress didn’t extend the federal subsidies enhancements that expired at the end of 2025, after-subsidy premiums increased sharply in 2026. And for West Virginia enrollees with household income above 400% of the federal poverty level, the return of the “subsidy cliff” (due to the expiration of the federal subsidy enhancements) is particularly challenging.
Source: CMS.gov11
Medicaid is another affordable health insurance option if you’re eligible. West Virginia expanded Medicaid under the ACA, so adults under age 65 are eligible for Medicaid with a household income up to 138% of the federal poverty level. Starting in 2027, however, there will be a Medicaid expansion work requirement.
How many insurers offer Marketplace coverage in West Virginia?
Two companies are offering 2026 individual and family plans through West Virginia’s exchange:4
- CareSource West Virginia Co.
- Highmark Blue Cross Blue Shield West Virginia
But CareSource is exiting West Virginia’s individual market at the end of 2026.13 Assuming no other carrier enters the Marketplace in West Virginia, residents will only be able to select a plan from Highmark BCBS for 2027.
West Virginia had only one participating insurer in its Marketplace in the first couple of years, but has had two for the last decade.14
Are Marketplace health insurance premiums increasing in West Virginia?
The following average premium changes were approved for West Virginia’s Marketplace insurers for 2026, amounting to a weighted average increase of 12% (but as explained below, after-subsidy premium increases were much larger than 12%).15
West Virginia’s ACA Marketplace Plan 2026 APPROVED Rate Increases by Insurance Company |
|
|---|---|
| Issuer | Percent Increase |
| CareSource West Virginia Co. | 7.6% |
| Highmark Blue Cross Blue Shield West Virginia | 13.9% |
Source: West Virginia SERFF16
The approved rates apply to full-price premiums, before subsidies are applied. It’s important to understand, however, that because Congress allowed the federal subsidies enhancements to expire at the end of 2025, after-subsidy premiums increased sharply in 2026, and some people lost their subsidies altogether. This is particularly challenging in a state like West Virginia, where full-price premiums are the highest in the country.11
For example, consider a 63-year-old couple in Cabell County, West Virginia, earning $85,000/year. That’s just over 400% of the 2025 federal poverty level, so this couple lost their entire subsidy at the end of 2025, and have to pay full price for their coverage in 2026. Here’s what that means for this couple:17
- 2025: The lowest-priced plan cost them $0/month.
- 2025: The lowest-priced Silver plan cost them $547/month, amounting to a little less than 8% of their income.
- 2026: The lowest-priced plan costs $3,039/month, amounting to 43% of their household income.
- 2026: The lowest-priced Silver plan costs $5,236/month, amounting to 74% of their household income.
For perspective, here’s an overview of how average full-price (unsubsidized) premiums have changed in West Virginia’s individual market over time (note that in years where multiple carriers offer plans, the averages may be unweighted as enrollment numbers in West Virginia filings are often redacted):
- 2015: Average increase of 10%.18
- 2016: Average increase of 24%.19 (second carrier began participating)
- 2017: Average increase of 45%.20
- 2018: Average increase of 25%.21
- 2019: Average increase of 9%.22
- 2020: Average increase of 7%.23
- 2021: Average increase of 5%. 24
- 2022: Average increase of 13%.25
- 2024: Average increase of 1.7%26
- 2025: Average increase of 7%27
How many people are insured through West Virginia’s Marketplace?
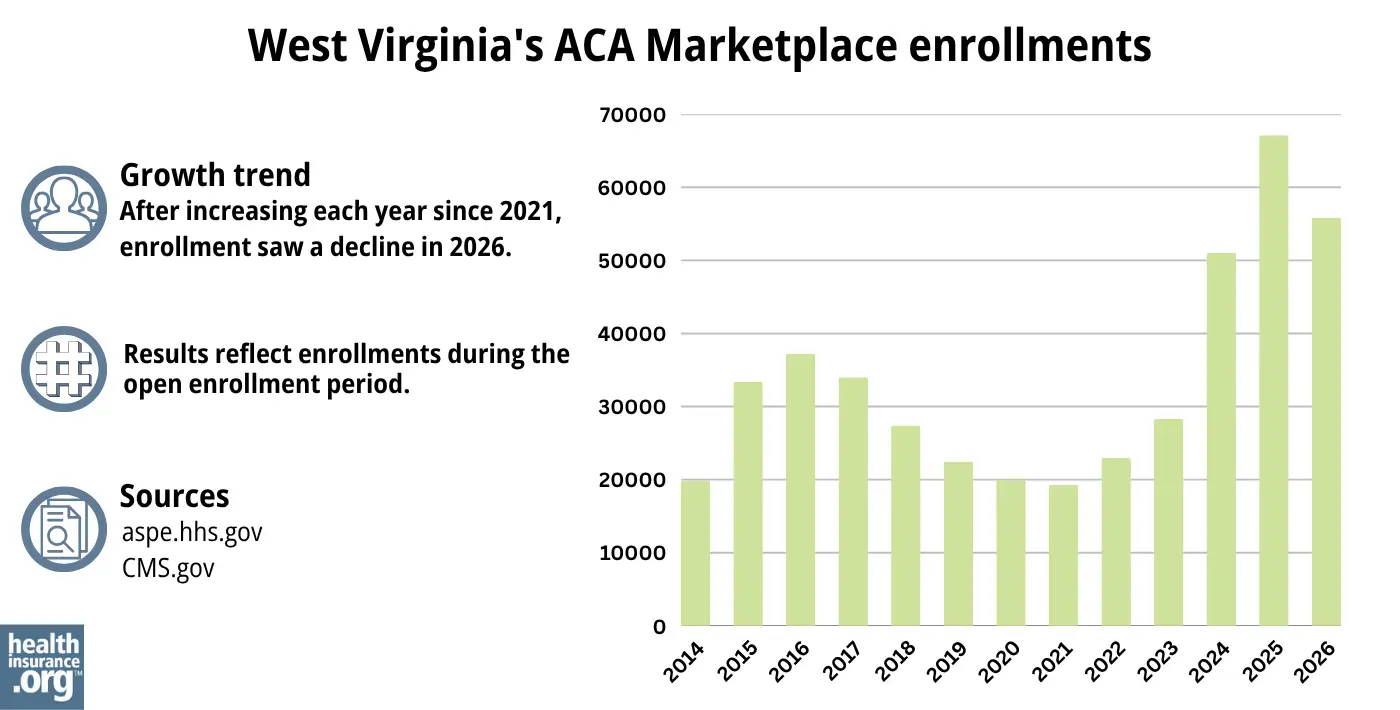
55,879 people enrolled in private plans through West Virginia’s Marketplace during the open enrollment period for 2026 coverage.28
That was down nearly 17% from the record high enrollment the year before, when 67,113 people selected plans during the open enrollment period for 2025 coverage.29
As illustrated below, West Virginia’s Marketplace enrollment had been climbing since 2022, largely due to the American Rescue Plan’s enhancements of the ACA’s premium subsidy rules. The Inflation Reduction Act extended the ARP’s subsidy enhancements through 2025. But they expired at the end of 2025, leading to the reduction in enrollments for 2026.
The enrollment growth in 2024 and 2025 was also driven by the “unwinding” of the pandemic-era Medicaid continuous coverage rule. CMS reported that nearly 29,000 people transitioned from Medicaid to a West Virginia Marketplace plan during the unwinding process.30
Source: 2014,31 2015,32 2016,33 2017,34 2018,35 2019,36 2020,37 2021,38 2022,39 2023,40 2024,41 202529 202642
What health insurance resources are available to West Virginia residents?
HealthCare.gov
This is the ACA Marketplace, where you can enroll in a health insurance plan online. You may also get help by calling (800) 318-2596.
West Virginia Offices of the Insurance Commissioner
Oversees and regulates insurance companies, brokers, and agents in the state while assisting consumers with insurance-related inquiries and concerns.
West Virginia Navigator
A free, non-profit program accessible to all residents within the state, providing free enrollment assistance.
West Virginia Senior Health Insurance Assistance Program (SHIP)
Helps answer questions and help Medicare beneficiaries.

Looking for more information about other options in your state?
Need help navigating health insurance options in West virginia?
Explore more resources for options in WV including short-term health insurance, dental, Medicaid and Medicare.
Speak to a sales agent at a licensed insurance agency.
Footnotes
- ”Marketplace 2026 Open Enrollment Period Report: National Snapshot” Centers for Medicare & Medicaid Services, Accessed March 2026 ⤶
- ”West Virginia Rate Review Submissions” RateReview.HealthCare.gov. Accessed Sep. 19, 2025 *The above is based on the most current data available. ⤶
- ”Marketplace 2026 Open Enrollment Period Report: National Snapshot” and “Marketplace 2025 Open Enrollment Period Report: National Snapshot” Centers for Medicare & Medicaid Services, Accessed March 2026 ⤶
- ”West Virginia Rate Review Submissions” RateReview.HealthCare.gov. Accessed Sep. 19, 2025 ⤶ ⤶
- Plan Year 2025 Qualified Health Plan Choice and Premiums in HealthCare.gov Marketplaces. Centers for Medicare and Medicaid Services. October 25, 2024. ⤶
- Medicare and the Marketplace, Master FAQ. Centers for Medicare and Medicaid Services. Accessed Oct. 29, 2025 ⤶
- Premium Tax Credit — The Basics. Internal Revenue Service. Accessed Oct. 29, 2025 ⤶ ⤶
- “When can you get health insurance?” HealthCare.gov. Accessed Mar. 10, 2026 ⤶
- “Find Local Help” localhelp.HealthCare.gov, Accessed Mar. 10, 2026 ⤶
- ”Entities Approved to Use Enhanced Direct Enrollment” CMS.gov, Apr. 7, 2026 ⤶
- “2026 Marketplace Open Enrollment Period Public Use Files” CMS.gov, March 2026 ⤶ ⤶ ⤶ ⤶
- “Federal Poverty Level (FPL)” HealthCare.gov, Accessed Sep. 19, 2025 ⤶
- ”SERFF tracking number CASO-134960415″ West Virginia SERFF. Accessed June 11, 2026 ⤶
- ”Number of Insurers Participating in the Individual Health Insurance Marketplaces” (West Virginia data). KFF.org. Accessed June 11, 2026 ⤶
- ”2026 Final Gross Rate Changes – West Virginia: +12.2% (updated)” ACA Signups. Oct. 28, 2025 ⤶
- ”West Virginia SERFF (tracking numbers CASO-134665901 and MSBC-134664604)” Accessed Oct. 29, 2025 ⤶
- ”See Plans & Prices” HealthCare.gov (zip code 25504, using 2025 and 2026 quoting). Accessed Oct. 29, 2025 ⤶
- Analysis Finds No Nationwide Increase in Health Insurance Marketplace Premiums. The Commonwealth Fund. December 2014. ⤶
- Highmark Blue Cross Blue Shield considered pulling out of Obamacare exchange. Metro News. November 2015. ⤶
- Avg. UNSUBSIDIZED Indy Mkt Rate Hikes: 25% (49 States + DC). ACA Signups. October 2016. ⤶
- West Virginia: 24.8% Rate Hikes; 10.9 Points Due To CSR Sabotage. ACA Signups. October 2017. ⤶
- 2019 Rate Hike Project Wrap-Up: FINAL/APPROVED Rate Changes For West Virginia. ACA Signups. November 2018. ⤶
- 2020 Rate Changes. ACA Signups. October 2019. ⤶
- 2021 Rate Changes. ACA Signups. October 2020. ⤶
- 2022 Rate Changes. ACA Signups. October 2021.[/efn-note]
- 2023: Average increase of 5%.[efn_note]West Virginia: Final Avg. 2023 #ACA Rate Changes: +5.0%. ACA Signups. October 2022. ⤶
- ”West Virginia: *Final* Avg. Unsubsidized 2024 #ACA Rate Changes: +1.7% (Unweighted)” ACA Signups. Nov. 8, 2024 ⤶
- ”West Virginia: Preliminary avg. unsubsidized 2025 #ACA rate changes: +7.0%” ACA Signups. Sep. 18, 2025 ⤶
- ”Marketplace 2026 Open Enrollment Period Report: National Snapshot” CMS Newsroom. March 2026 ⤶
- “2025 Marketplace Open Enrollment Period Public Use Files” CMS.gov, May 2025 ⤶ ⤶
- ”HealthCare.gov Marketplace Medicaid Unwinding Report” Centers for Medicare & Medicaid Services. Data through April 2024; Accessed Aug. 5, 2024 ⤶
- “ASPE Issue Brief (2014)” ASPE, 2015 ⤶
- “Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report”, HHS.gov, 2015 ⤶
- “HEALTH INSURANCE MARKETPLACES 2016 OPEN ENROLLMENT PERIOD: FINAL ENROLLMENT REPORT” HHS.gov, 2016 ⤶
- “2017 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2017 ⤶
- “2018 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2018 ⤶
- “2019 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2019 ⤶
- “2020 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2020 ⤶
- “2021 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2021 ⤶
- “2022 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2022 ⤶
- “2023 Marketplace Open Enrollment Period Public Use Files” CMS.gov, March 2023 ⤶
- ”HEALTH INSURANCE MARKETPLACES 2024 OPEN ENROLLMENT REPORT” CMS.gov, 2024 ⤶
- “2026 Marketplace Open Enrollment Period Public Use Files” CMS.gov, May 2025 ⤶

