Tennessee Health Insurance Marketplace for 2026

Compare ACA plans and check subsidy savings from a licensed third-party health insurance agency.
Tennessee Marketplace quick facts
Tennessee health insurance Marketplace guide
This guide, including the FAQs below, was developed to assist you in choosing the right Tennessee health insurance plan for you and your family. The options found in Tennessee’s ACA Marketplace may be a good choice for many consumers, and we will guide you through the options below.
Tennessee uses the federally-facilitated health insurance exchange (Marketplace), HealthCare.gov, for residents to purchase its ACA Marketplace plans. The Tennessee Marketplace provides access to health insurance products from six private insurers for 2026 (see below for details about 2026 premium changes).4 All six insurers also offered coverage for 2025.5 But plan availability varies from one area of the state to another.
When you enroll in a plan through the Marketplace, you may find that you’re eligible for financial assistance that reduces the monthly cost of your coverage (premium subsidies), and possibly also your out-of-pocket expenses (cost-sharing reductions, or CSR). These are federal subsidy programs created by the Affordable Care Act, and eligibility depends on your income and circumstances.
Frequently asked questions about health insurance in Tennessee
Who can buy Marketplace health insurance in Tennessee?
To qualify for health coverage through the Tennessee Marketplace, you must:6
- Live in Tennessee
- Be lawfully present in the United States
- Not be incarcerated
- Not be enrolled in Medicare
Eligibility for financial assistance (premium subsidies and cost-sharing reductions) depends on your income. In addition, to qualify for financial assistance with your Marketplace plan you must:
- Not have access to affordable employer-sponsored health insurance. If your employer offers coverage but you feel it’s too expensive, you can use our Employer Health Plan Affordability Calculator to see if you might qualify for premium subsidies in the Marketplace.
- Not be eligible for Medicaid or CHIP.
- Not be eligible for premium-free Medicare Part A.7
- Not be able to be claimed by someone else as a tax dependent.8
- If you’re married, you must file a joint tax return with your spouse.8 (with very limited exceptions)9
When can I enroll in an ACA-compliant plan in Tennessee?
In Tennessee, the open enrollment period for 2026 individual/family health coverage ended on January 15, 202610
The next open enrollment period, for 2027 coverage, will be shorter. It will run from November 1, 2026 to December 15, 2026. And all plans selected during open enrollment will take effect on January 1. The shorter open enrollment period is due to a federal rule change that took effect in 2025.
Outside of open enrollment, a special enrollment period (typically triggered by a specific qualifying life event) is necessary to enroll or make changes to your coverage.
If you have questions about open enrollment, you can learn more in our comprehensive guide to open enrollment. We also have a comprehensive guide to special enrollment periods.
How do I enroll in a Tennessee Marketplace plan?
To enroll in an ACA Marketplace plan in Tennessee, you can:
- Visit HealthCare.gov to access Tennessee’s health insurance marketplace. Here you will find an online platform to shop, compare, and choose the best health plans.
- Purchase individual and family health coverage with the help of an insurance agent or broker, a Navigator or certified application counselor, or an approved enhanced direct enrollment entity.11
You can also call HealthCare.gov’s contact center by dialing 1-800-318-2596 (TTY: 1-855-889-4325). The call center is available 24 hours a day, seven days a week, but it’s closed on holidays.
How can I find affordable health insurance in Tennessee?
Tennessee uses the federally facilitated exchange for individual market plans, so residents who buy their own health insurance enroll through HealthCare.gov.
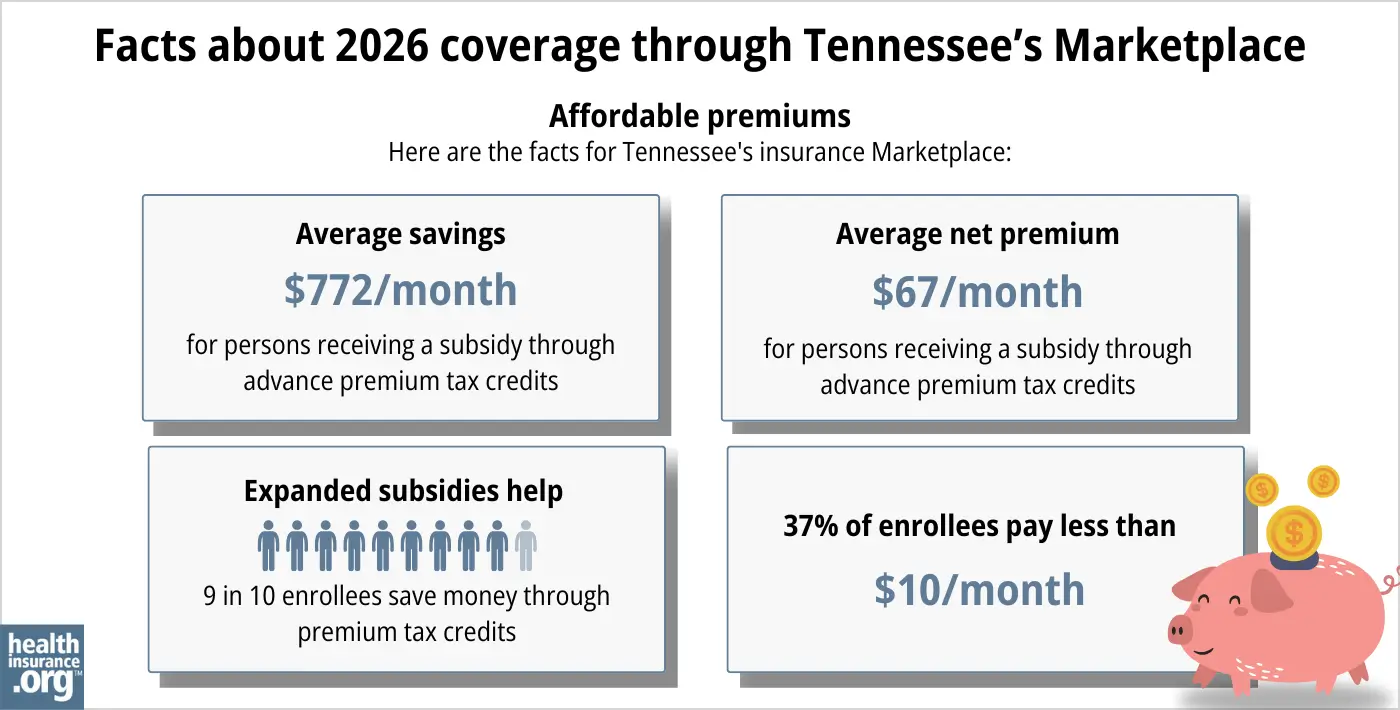
Ninety percent of the people who purchased health plans through the Tennessee Marketplace during the open enrollment period for 2026 coverage were eligible for advance premium tax credits (APTC), also known as premium subsidies. The APTC amounted to an average savings of $772/month and reduced the average subsidy-eligible enrollee’s premium to about $67/month.1
But because Congress didn’t extend the federal subsidy enhancements that expired at the end of 2025, subsidies are no longer available to enrollees who earn more than 400% of the federal poverty level, and subsidies don’t cover as much of total premiums as they did in 2025.
Source: CMS.gov1
Marketplace enrollees with household incomes of no more than 250% of the federal poverty level also qualify for cost-sharing reductions (CSR) that will result in lower deductibles and out-of-pocket expenses for Silver plans (these cost-sharing reductions are not available on plans at other metal levels).12 Between the premium subsidies and cost-sharing reductions, you may find that a Tennessee Marketplace health insurance plan provides the best value.
Tennessee has a coverage gap because the state has refused to expand Medicaid under the Affordable Care Act. Childless adults without disabilities are ineligible for Tennessee Medicaid regardless of how low their income is. Because the ACA’s premium tax credits (subsidies) aren’t available to applicants with income below the poverty level (because the law called for them to have expanded Medicaid instead), these applicants fall into what’s come to be known as a coverage gap. They are ineligible for Medicaid and also ineligible for premium tax credits to make private coverage more affordable.
There are an estimated 82,000 Tennessee residents in the coverage gap.13
But starting in mid-2024, Tennessee closed the coverage gap for low-income parents of minor children. This population is now eligible for Medicaid with an income up to the poverty level, and Marketplace subsidy eligibility begins above that point.
How many insurers offer Marketplace coverage in Tennessee?
For 2026 coverage, six insurers offer individual/family health plans through the exchange/Marketplace in Tennessee,4 all of which also offered coverage for 2025:5
- Blue Cross Blue Shield of Tennessee
- Cigna
- Oscar
- Celtic/Ambetter
- UnitedHealthcare
- Alliant Health Plans
Plan availability varies from one part of the state to another, as insurers have differing coverage areas.
Are Marketplace health insurance premiums increasing in Tennessee?
For 2026, the following average rate changes were approved for Tennessee’s Marketplace insurers,14 amounting to a weighted average rate increase of 37.5% for full-price (pre-subsidy) premiums:15
Tennessee’s ACA Marketplace Plan 2026 APPROVED Rate Increases by Insurance Company |
|
|---|---|
| Issuer | Percent Increase |
| Blue Cross Blue Shield of Tennessee | 42.1% |
| Cigna | 40.1% |
| Oscar | 35.5% |
| Celtic/Ambetter | 37.2% |
| UnitedHealthcare | 30.2% |
| Alliant Health Plans | 10.8% |
Source: Federal rate review database14
Tennessee no longer has an effective rate review program, so the federal government (CMS) reviews the rates that are filed in Tennessee.16
The average approved rate changes listed above are calculated before any subsidies are applied. The majority of Tennessee’s Marketplace enrollees do receive subsidies, which generally change each year to keep pace with the cost of the second-lowest-cost Silver plan in each area.
But because Congress didn’t extend the federal subsidy enhancements that had been in effect since 2021, they expired at the end of 2025. Because the subsidy enhancements expired, subsidies no longer cover as much of enrollees’ premiums, and aren’t available to as many people. This resulted in Marketplace coverage becoming much less affordable than it was in 2025.
For perspective, here’s an overview of how full-price (unsubsidized) average premiums have changed in Tennessee over the years:
- 2015: Average increase of 9%.17
- 2016: Average increase of 28.2%.18
- 2017: Average increase of 56%.19
- 2018: Average increase of 28.5%.20
- 2019: Average decrease of 12.4%.21
- 2020: Average decrease of 1.1%.22
- 2021: Average increase of 8.2%23
- 2022: Average increase of 4.4%.24
- 2023: Average increase of 8.5%.25
- 2024: Average increase of 4.8%.26
- 2025: Average increase of 1.4%5,27
How many people are insured through Tennessee’s Marketplace?
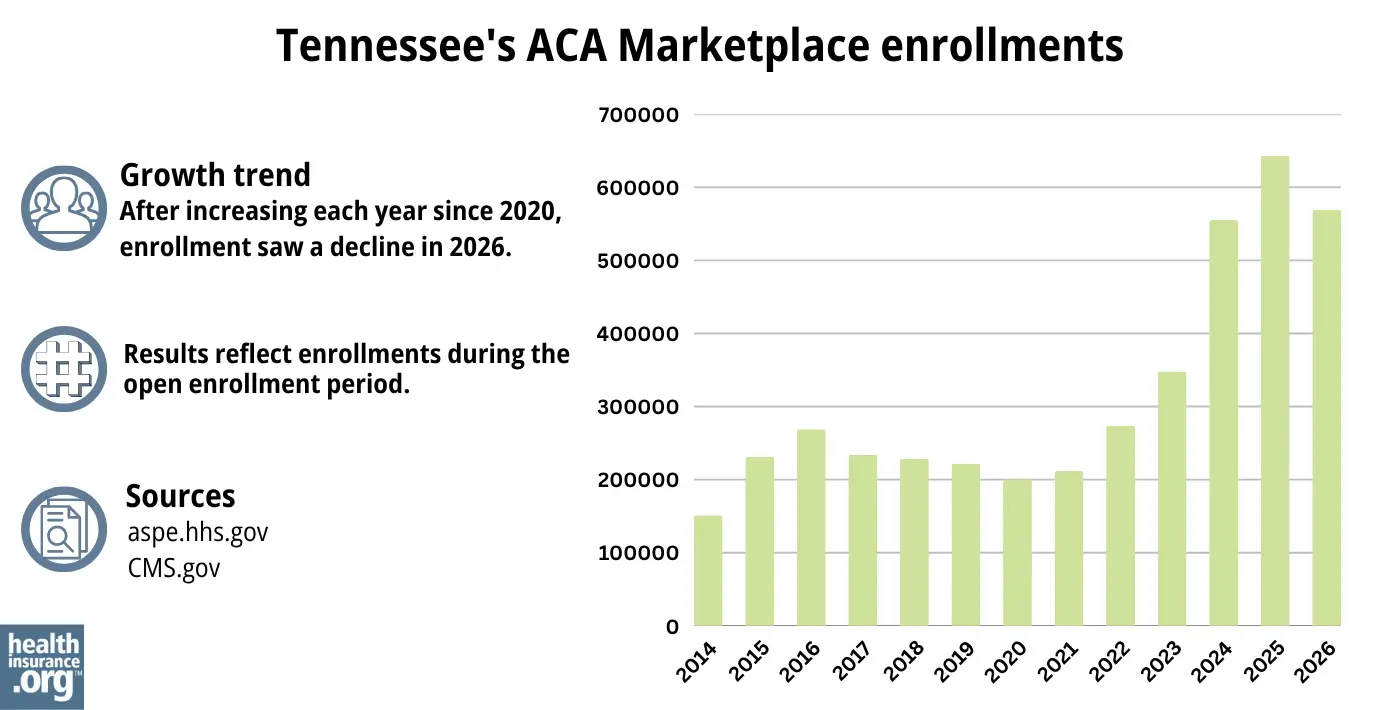
569,310 people selected plans through the Tennessee Health Insurance Marketplace during the open enrollment period for 2026 coverage.[1
This was a drop of more than 11% from the year before, when a significant record-high of 642,867 people enrolled through the Tennessee exchange during the open enrollment period for 2025 coverage.28 (See chart below for a summary of enrollment by year.)
Source: 2014,29 2015,30 2016,31 2017,32 2018,33 2019,34 2020,35 2021,36 2022,37 2023,38 2024,39 202528 20261
The surge in enrollment in recent years was due in part to the American Rescue Plan (ARP) making ACA’s premium subsidies more substantial. Under the ARP’s subsidy enhancement rules – extended through 2025 by the Inflation Reduction Act – subsidies became larger and more widely available than they had been prior to 2021.40 But because Congress let these subsidy enhancements expire at the end of 2025, Marketplace coverage became significantly more expensive in 2026, and fewer people enrolled.
The enrollment growth for 2024 and 2025 was also due in part to the “unwinding” of the COVID-related Medicaid continuous coverage rule (people were not disenrolled from Medicaid for three years during the pandemic, but that ended in the spring of 2023). Nearly 124,000 Tennessee residents transitioned from Medicaid or CHIP to a private Marketplace plan during the unwinding period.41
What health insurance resources are available to Tennessee residents?
HealthCare.gov
800-318-2596
Tennessee Insurance Division
Oversight of the plans sold in the Tennessee Marketplace
State Exchange Profile: Tennessee
The KFF overview of Tennessee’s progress toward creating a state health insurance exchange.

Looking for more information about other options in your state?
Need help navigating health insurance options in Tennessee?
Explore more resources for options in TN including short-term health insurance, dental, Medicaid and Medicare.
Speak to a sales agent at a licensed insurance agency.
Footnotes
- ”2026 Marketplace Open Enrollment Period Public Use Files” CMS.gov. April 2026 ⤶ ⤶ ⤶ ⤶ ⤶
- ”Tennessee Rate Review Submissions” RateReview.HealthCare.gov. Accessed Sep. 21, 2025 *The above is based on the most current data available. ⤶
- ”2026 Marketplace Open Enrollment Period Public Use Files” and “Marketplace 2025 Open Enrollment Period Report: National Snapshot” Centers for Medicare & Medicaid Services, April 2026 ⤶
- ”Tennessee Rate Review Submissions” RateReview.HealthCare.gov. Accessed Sep. 21, 2025 ⤶ ⤶
- ”TDCI Offers Consumer Insurance Tips for 2025 ACA Open Enrollment” Tennessee Department of Commerce and Insurance. October 31, 2024. ⤶ ⤶ ⤶
- ”A quick guide to the Health Insurance Marketplace” HealthCare.gov ⤶
- Medicare and the Marketplace, Master FAQ. Centers for Medicare and Medicaid Services. Accessed Jan. 7, 2026 ⤶
- Premium Tax Credit — The Basics. Internal Revenue Service. Accessed Jan. 7, 2026 ⤶ ⤶
- Updates to frequently asked questions about the Premium Tax Credit. Internal Revenue Service. February 2024. ⤶
- “When can you get health insurance?” HealthCare.gov. Accessed Jan. 7, 2026 ⤶
- “Entities Approved to Use Enhanced Direct Enrollment” CMS.gov. Dec. 8, 2025 ⤶
- ”APTC and CSR Basics” Centers for Medicare & Medicaid Services. Accessed February 15, 2024. ⤶
- How Many Uninsured Are in the Coverage Gap and How Many Could be Eligible if All States Adopted the Medicaid Expansion? KFF. Feb. 25, 2025 ⤶
- ”Tennessee Rate Review Submissions” RateReview.HealthCare.gov. Accessed Jan. 7, 2026 ⤶ ⤶
- ”2026 Final Gross Rate Changes – Tennessee: +37.5% avg; ~555,000 enrollees are in for a hell of a shock this fall (updated)” ACA Signups. Nov. 1, 2025 ⤶
- ”State Effective Rate Review Programs” CMS.gov. Accessed Mar. 13, 2026 ⤶
- Analysis Finds No Nationwide Increase in Health Insurance Marketplace Premiums. The Commonwealth Fund. December 2014. ⤶
- FINAL PROJECTION: 2016 Weighted Avg. Rate Increases: 12-13% Nationally* ACA Signups. October 2015. ⤶
- 2017 Rate Project State Roundup: IN, IA, ME, MA, MT, ND, SD, TN. ACA Signups. September 2016. ⤶
- 2018 Rate Hikes. ACA Signups. October 2017. ⤶
- Tennessee: Correction Re. Final 2019 #ACA Rate Changes: 12.4% DROP (Vs. ~22% Drop W/Out #ACASabotage). ACA Signups. October 2018. ⤶
- Tennessee: APPROVED Avg. 2020 #ACA Premiums: 1.1% DECREASE; 3 Carriers Expanding Coverage. ACA Signups. August 2019. ⤶
- Weighted average calculated by healthinsurance.org, using these sources: TDCI Approves Health Insurance Carriers’ Rates on the Federally Facilitated Marketplace for 2021. Tennessee Department of Commerce and Insurance. September 2020. And Tennessee: Preliminary Avg. 2021 #ACA Premiums: +5.0% Indy Market, +5.5% Sm. Group. ACA Signups. July 2020. ⤶
- Tennessee: Approved Avg. 2022 #ACA Rate Changes: +4.4% Indy Market; +8.9% Sm. Group (Updated). ACA Signups. October 2021. ⤶
- Tennessee: Final Avg. Unsubsidized 2023 #ACA Rate Changes: +8.5%. ACA Signups. October 2022. ⤶
- Tennessee: *Final* Avg. Unsubsidized 2024 #ACA Rate Changes: +4.8%. ACA Signups. September 2, 2023. ⤶
- “Tennessee: Preliminary avg. unsubsidized 2025 #ACA rate changes: +1.4% (unweighted); Alliant & Ascension leaving?” ACA Signups. Sep. 13, 2024 ⤶
- “2025 Marketplace Open Enrollment Period Public Use Files” CMS.gov, May 2025 ⤶ ⤶
- “ASPE Issue Brief (2014)” ASPE, 2015 ⤶
- “Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report” HHS.gov, 2015 ⤶
- “Health Insurance Marketplaces 2016 Open Enrollment Period: Final Enrollment Report” HHS.gov, 2016 ⤶
- “2017 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2017 ⤶
- “2018 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2018 ⤶
- “2019 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2019 ⤶
- “2020 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2020 ⤶
- “2021 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2021 ⤶
- “2022 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2022 ⤶
- “2023 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2023 ⤶
- ”HEALTH INSURANCE MARKETPLACES 2024 OPEN ENROLLMENT REPORT” CMS.gov, 2024 ⤶
- “Health Insurance Marketplaces 2023 Open Enrollment Report” CMS.gov, 2023 ⤶
- ”HealthCare.gov Marketplace Medicaid Unwinding Report” Centers for Medicare & Medicaid Services. Data through April 2024; Accessed Aug. 2, 2024 ⤶

