






EDITOR’S NOTE: Healthinsurance.org’s Curbside Consult is a periodic informal dialogue with medical and health policy experts about pressing issues of the day.

Avik Roy, author of “Transcending Obamacare,” left, and Curbside Consult Host Harold Pollack
Avik Roy’s 20,000-word health reform plan – “Transcending Obamacare” – is one of the few conservative proposals that spells out how Republicans might push the Affordable Care Act in a more conservative direction.
In our final interview segment, we focus heavily on coverage for low-income Americans and how we should and could be delivering better benefits and access. It’s no secret that Avik isn’t a fan of Medicaid; he says it offers the “false promise” of coverage. And in his proposal, the safety net would be phased out by ‘migrating’ virtually everyone – including low-income populations – to the same exchange-based system.
The competitive pressures of the exchanges, Roy says, provides higher-quality and more cost-effective benefits for “roughly the same costs as the Medicaid benefit.” I’ll let readers make that call. In my view, Roy greatly understates the value of Medicaid coverage.
A great irony of health reform is that exchange-heavy Medicaid plans such as Arkansas’ “private option” have become the negotiating stance used by Republican state officials to politically differentiate their proposals from Obamacare. Shift the facts slightly, and one can imagine something like the Arkansas plan being the basic liberal position, with Republican governors demanding to place low-income people into traditional Medicaid to save money. Whatever. If this negotiation accelerates the path to near-universal coverage, I’m all in for it.
I hope you’ve enjoyed our conversation.
Watch Part 1 of this interview.
Watch Part 2 of this interview.
Transcript of Part 3 (of 3):
Better insurance for low-income Americans
Harold: Let’s go to Medicaid. You are very critical of Medicaid, you’ve written quite a bit attacking Medicaid as promoting worse health outcomes than other forms of insurance. I think you and I would agree that the low provider reimbursement in Medicaid is a really serious problem.
Avik: Yeah and this is one of the things that I really try to … one of my highest priorities in how I designed this plan was to attack that problem … the problem of poor health outcomes and poor quality of health coverage for low-income Americans. You and I and have had this argument in the past and I think the straw man that’s always assigned to me is: “Well you don’t like Medicaid so you just want the poor to die in the streets.”
I’ve always insisted, that “No that’s not what I want.” And now I’ve had the opportunity to demonstrate that. What I’m proposing here, is actually … I would contend … a substantially better insurance benefit for low-income Americans. Why? As I said before, the HSA component allows them to actually save for their own needs, their own financial and health needs and over time build a real nest egg, build actual wealth instead of being completely dependent on a system forever. I think that is very important, very attractive.
Secondly, based on our modeling … so as you may know from a plan, there is a metric we use to actually measure provider access and health productivity … that is to say … a proxy for health outcomes. Because I was very concerned about making sure that we could actually improve the quality of health coverage for the poor. So how do we do that?
Moving from Medicaid to exchange-based coverage
Because they would be on exchange-based coverage in which the networks and the physician acceptance is broader, there would be a substantial increase … nearly double, based on these indices … of access to physicians and also the access to health care services relative to the Medicaid program. I’m trying to find the table. Here we go. It’s table one, page 19 of the plan that describes some of these details. That’s something that’s very important. And the HSA components are a big part of this, because what is it that the typical low income person really needs?
Yes there are the cases of people who’ve got high consumption of health care and are just basically looking for a funding source. But if you think about the typical low-income person, a typical low income person has one or more of the following conditions: high blood pressure, high cholesterol, diabetes, smoking, poor health maintenance, food deserts and problems like that. What is the common thread in all those problems?
It’s not actually expensive health care services. The pharmaceuticals that treat diabetes, high blood pressure, high cholesterol are all generics. They’re all extremely cheap. They would cost less than a bottle of Coke but what these people don’t have is access to primary care physicians.
If you give people the flexibility to take their HSA money say and invest that in a high-quality primary care … which they certainly could do with that level of support … they could do a lot to actually have high-quality nutritional support, high-quality primary care and high-quality management of their chronic diseases. That’s what the vast majority of low-income people need.
I think Paul Ryan’s anti-poverty plan has been mocked because it involves life coaches and some other things like that. Well it’s easy to mock, but at the end of the day that’s what it is that a lot of low-income people don’t have … is people who are actually on a human level looking out for them. It’s easy to throw money at a problem. It’s a lot harder to actually have actual human beings who are skilled to look out for people.
Battling low reimbursement rates
Harold: Let me jump in. First of all it’s hard to throw money at a problem that affects a marginalized constituency especially when we leave it to state governments to make some of these critical decisions. Medicaid … the problem of low reimbursement is a problem that is a state government policy decision that they have made …
Avik: Well, yes and no, let me just say one thing about that because this is an important point. So why is it that that states reduce reimbursement rates for doctors and hospitals? It’s because it’s the only policy tool they really have to keep their fiscal commitments and check in the Medicaid program because everything else is prohibited by the Medicaid statute.
So they can’t change the copays, they can’t change the premiums … There’s so little they can do and anything they possibly can do, they have to apply for 1115 waiver that takes three years, and it will probably be rejected anyway.
So what’s the tool that’s at their disposal? It’s lowering reimbursement rates.
Federalizing acute-care set-up
The whole point of this approach is to say let’s federalize the acute-care set-up … and so that way, the federal government is defining the benefit. It’s funding the benefit and in that way the states don’t really have a role in that problem and it’s also taken off their hands.
So under this approach the state governments have no role in funding acute-care Medicaid … and they can focus on just regulating the insurance companies as an additional layer obviously on top of the federal regulations, but they won’t have to worry. The reimbursement rates will be determined by the competitive marketplace that everyone else is in.
Harold: Let me say a couple of things about that. One is … states actually have more flexibility on Medicaid than you’ve just let on. Many states have … you know … Medicaid managed care is a very large percentage of … certainly of the acute-care Medicaid insurance group that you are talking about. Insurance companies that participate in Medicaid managed care can set all sorts of reimbursement rates within the existing system. There’s actually tremendous variation.
I do think relying on state governments to provide basic services to vulnerable people is a huge problem. It is the reason Medicare is federalized and Medicaid we leave so much to the states. It’s because seniors are a more powerful constituency than the traditional Medicaid recipients are. So I worry about that.
In fact, one of the components of your plan to give state governments responsibility for long-term care … I think at least we would have to think very carefully about how to do that. Knowing that you are backed by the full faith credit of the state of Illinois in your long-term care needs … that’s a little scary.
Migrating everyone to same system
Avik: Let me make a couple points about that. So first on the acute-care side … this is really important: Remember the acute-care side of this is all being funded by the federal government. The federal government would provide the guarantee. The state’s role is as the regulator of state-based insurance companies, to make sure the insurance companies are not doing bad stuff.
But there is also again a federal layer of insurance as well … and what’s more important than that is that you have made this point about the marginalization of health coverage for poor people and low-income people.
One of the great attractions of migrating everyone to same system over time … the Medicaid population, the individual market, the exchange population, the younger retirees over time, plus some people who would come out of the employer-sponsored system and shop for coverage on their own … you would have so many people in that system that it wouldn’t just be low-income people campaigning for higher quality coverage in the exchanges. It would be a large subset of the U.S. population, including some of those politically active and wealthier constituencies that you refer to.
I think if you want poor people to get better coverage, one political economy tool if you have to make that happen is to integrate them into the same kind of coverage that other people in the health care system enjoy and do very well with.
As we know from the recent study by Sommers and colleagues in Massachusetts, the exchange-based plans have done fairly well in terms of improving health outcomes for the low-income population. So all this is to say that I agree with you that there are a lot of problems with Medicaid.
I’m trying actually to consider those problems and do something about them. This is not a plan that ignores or neglects the problems you described, but a plan that actually quite directly and intentionally tries to remedy those problems and address them. So that’s on the acute-care side.
Ensuring meaningful coverage benefits
Harold: Let me make a couple of comments about that. The first thing is … a lot depends on how we set up the exchanges. If we set up the exchanges so that the populations really separate and poor people end up in a set of plans that are quite different from the plans that other people go in. For example if you have economical plans with narrow networks that low-income people tend to gravitate to …
Avik: They would have no incentive to do that … right? … because they would have subsidies that would be benchmarked to a fairly generous actuarial value. So they wouldn’t have an incentive to choose … I mean … they would choose a lower plan and I suppose keep the savings if they wanted to in a HSA deposit … I mean you could design it that way. The idea here is that low-income people would have a pretty meaningful insurance coverage benefit.
And again if you look at the way the ACA setup works, typically the people who are eligible for subsidies are choosing more generous coverage than the unsubsidized population. So among the subsidy-eligible population, almost everyone is choosing a silver plan. Among the unsubsidized population almost everybody is choosing the bronze plan.
It’s kind of the inverse of what you are describing. So I think we have a lot of evidence that if you subsidize the premium product that, of course, classical economics would teach you makes people less sensitive to the price of the plan and therefore they are going to choose a more generous coverage benefit.
Can problems be addressed within ACA?
Harold: That is … I would just say … one of the things we would have to watch as it moves forward. I do think, from a progressive perspective … many of the problems you identify we could deal with right now within the structure of ACA. For example, ACA went some distance to raise primary care reimbursement rates for some period of time. I wish that were more generous.
There’s a bunch of things we could do to raise reimbursement rates in Medicaid just within the current structure right now … and it’s really a political question at both the state and the federal level: Are we willing to spend the money to do that? And if we are not willing to spend the money to do that within the existing structure, I think we are going to see that politics will recreate itself in some fashion over time. That concerns me a lot.
We obviously … if we said we really need to get everybody in Medicaid into a good primary care situation, we could do that right now … if we were committed to doing it. It’s not particularly expensive. One of the things that striking in Illinois is we spend half of our Medicaid budget on 3 percent of the people. If we wanted to provide much nicer benefits to the bottom 80 percentage of the recipients, we could do that. We just choose not to do that.
Avik: Well underlying your set of assertions there is that Medicaid as currently structured is equally as efficient, both in terms of the cost and quality, as exchange-based coverage would be … and I would simply disagree with that. I think the exchange-based coverage is more cost-efficient over the long run, because the competitive dynamics are such that they drive lower prices and more quality and innovation, cost innovation, and higher quality.
Harold: What is the evidence for lower prices? It seems to me that …
Competitive pressures created by exchanges
Avik: I cited you some of the evidence from Medicare Advantage and we also have evidence from Arkansas. Arkansas has a situation where they’ve got so-called private option which is far more constrained, by the way, than what I’m proposing in terms of true exchange benefit because it is an exchange benefit plus Medicaid wrap-around. So it’s not as efficient in that sense as a true exchange base plan would be.
But there, they’re showing … if results from the state government are to be believed … some reason to be cautiously optimistic that the so called “private option” which everyone believed, including myself, would be very, very expensive for that Medicaid population may be less expensive than people thought. And we are certainly seeing in the 2015 round of rate increases or rate decreases in the overall of exchanges across the country that the rate increases are relatively in line with broader health cos trends.
I think there’s a lot of reason to be optimistic that the competitive pressures of the exchange creates can do a lot to create a higher-quality, more cost-efficient benefit and again I think one thing I would emphasize here is that this model shows that for roughly the same cost as the Medicaid benefit … the current Medicaid spending and Medicaid benefit … we are getting dramatically higher access.
Your argument is “Well, yeah … we can address this problem by spending a lot more money on Medicaid” but if we could get the same level of provider access and the same level of quality by spending the same amount of money, why wouldn’t we want to do that instead?
Harold: By the way, one of the things I like about the Arkansas approach … one of the reasons by the way why I think it’s had a good financial projection … is that the group of people that they are applying the private options to has been well chosen. They’ve been careful. There are various avenues out of being put into the exchange for people with specific issues and they’ve been very careful.
Avik: Yeah, it leans a little healthier than the overall Medicaid population. That’s why I say I’m cautious but optimistic about what Arkansas is doing.
Shouldn’t we be feeling better about the ACA?
Harold: By the way I’m very happy with the way ACA is going. After the initial disaster with HealthCare.gov, things are going very well right now. One of the reasons why I’m feeling that … and I have contradictory feelings … One is this not a great moment to compromise because things are going well, but the other is … politically, things on the ground are going very well, but the politics of ACA are not particularly going well.
And I think both Democrats and Republicans have to realize this isn’t 2008 and it’s not 2010 either. We have actually a very successful set of thin gs happening in ACA. Republican governors and the Obama administration and others are starting to realize that we really have to start talking seriously about … This thing has happened on the ground. It’s a reality. How are we going to work together to make it better and to achieve our different … sometimes conflicting but sometimes consistent … objectives so that this thing is actually working well 15 years from now?
I don’t know how you are feeling about ACA but I’m feeling very good about what’s happened. Once the exchange has gotten up and running, you look at the rate increases, you look at the reduction in the uninsured in places like Arkansas and Kentucky. The human story there is really quite moving.
Avik: Well, I would vigorously contest the argument that the ACA is going well. I’d say, the ACA is going well for the beneficiaries of the ACA. It’s not going well for the people whose rates have sky rocketed, it’s not going well for the people who’ve lost jobs because of the higher cost of hiring because of the employer mandate, people whose jobs have been moved from full time to part time. I think there are plenty of people who are losers in the law and there are plenty of people who are winners.
An we can have an energetic debate about whether those tradeoffs are worth it. But I think a complete and fair understanding and contextual understanding of the ACA from both sides frankly would take into account both the winners and losers. And I think what the left does is it celebrates the winners and ignores the losers. What the right does is it highlights the losers and ignores the winners.
I think if you take the whole sweep of it, I think the fairest way to put it there are losers and there are winners. The goal of future reform efforts from either side should be to mitigate what happens with the losers and try to preserve the benefits for the winners.
Harold: Now let me ask you this … I think that’s a fair point I think … By the way we didn’t talk about the employer mandate but ti think that is an area where … I don’t particularly identify with the employer mandate. I think many of us on the liberal side would be happy to see some sort of relaxation of it now that the exchanges are working well.
Why lower the federal poverty level cut-off?
Avik: Can I make one quick point related to that because it reminds us of what we talked before? You mentioned that I bring down the subsidy threshold from 400 percent of FPL to 317 percent of FPL.
Harold: That’s the federal poverty level.
Avik: That was done for some specific policy reason. In Massachusetts, they achieved near universal coverage with a 300 [percent] FPL threshold in a state that obviously had a relatively low un-insurance rate to begin with.
But still, the meaningful reduction that everyone sees as a model came from a 300 percent FPL threshold. The Congressional Budget Office has actually modeled this out, as have a number of independent places like the Urban Institute, who have said that if you actually reduce the threshold from 400 percent to 300 percent of FPL, the coverage impact is minimal, because most of the people who are in the 300 to 400 percent FPL income level have employer-sponsored coverage.
So I go with 317 because that is just a smoother graduation of the subsidies. But the idea there is that you want subsidize and direct the resources toward the people who really need the help, not to people who don’t need the help.
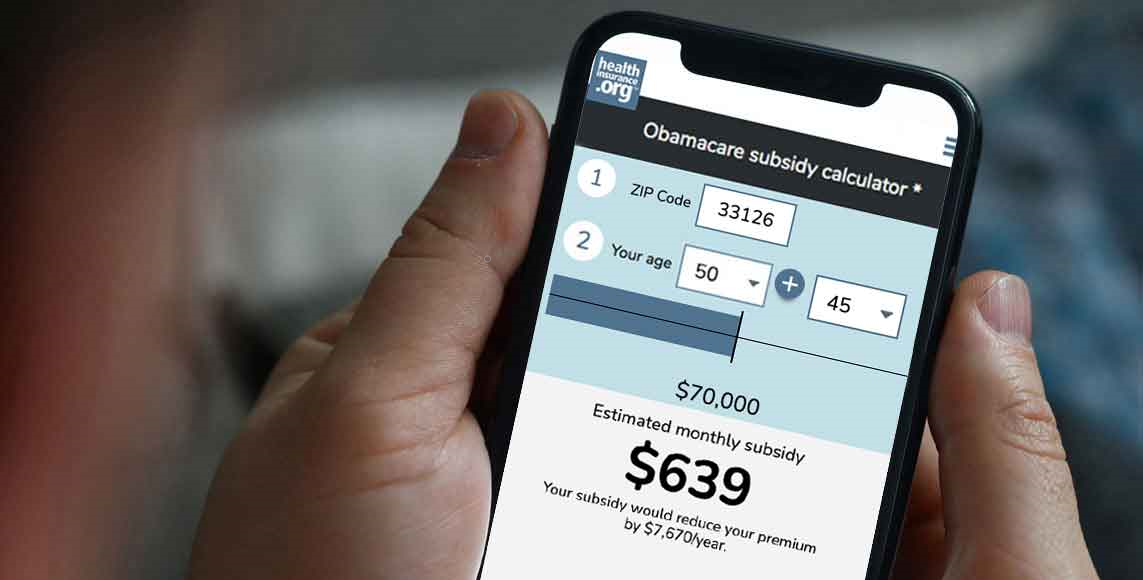
Harold: By the way just for people that aren’t FPL experts … that’s the federal poverty line. For a family of four, 300 percent of FPL is something like $70,000 … something in that range.
Avik: It’s like $90,000 I think for a family of four.
Harold: Well, we will get the correct number, so people have the sense magnitudes.
(NOTE FROM HAROLD POLLACK: The correct figure is, indeed, about $71,550.)
One of the communication failures in the conversation with the ACA was to do so much discussion … We would explain … there are so many people who are totally eligible for subsidies in under ACA who have no idea … who think it’s for other people because they don’t know what the federal poverty line is and that they’re at 322 percent of it.
There is one thing … one thing I like about your plan is near universal coverage. The one tragic thing for me right now is … where I started. Actually, my first campaigning for candidate Obama was calling on the phone rural African Americans in South Carolina, telling them about this Senator Obama guy. Why they had me doing that … since these are of course my people … I don’t know. That is the mystery of campaigning.
And I talked to … I remember talking to an older gentleman with diabetes and he was talking to me about how his wife had health problems. And he basically said: “If your guy wins, will he help me?” It was like a punch in the stomach, because it wasn’t like: “Do you have a Will.i.am video that you can send me?” This was like: “I’ve got some bills right now …”
As you and I know, the best benefit … the most immediate benefit that the Medicaid extension brings to people … is basic financial security and mental health … which you should put into your thing by the way, in your discussion of Oregon.
And I thought, you know, when ACA passed, I thought of that guy. I thought: You know I helped that guy … because I didn’t know whether I was just BS-ing him when I said yeah we are going to help you or not. And then the Supreme Court struck and all these red-state conservative governors were rejecting the Medicaid expansion … have shut out poor people who are not their voters, often are non white and were stuck. What can we do about that?
Medicaid: A ‘false promise’?
Avik: Well, as you know Harold, I wrote a book entitled, “How Medicaid fails the poor” … so I’ve taken much dimmer view than you of the degree to which a low-income person with diabetes benefits from the Medicaid program. And I think that what I really am energized by with my plan is that I can go to that individual, and really … with great confidence … say that this plan is better for that individual than the ACA, because Medicaid is a false promise.
It’s a card that gives you the false sense that you have coverage but it doesn’t actually give you the care you need when you need it … and that’s something that I spent an enormous amount of time and an enormous amount of work trying to change, and being very careful and working really hard because of all the tradeoffs and health care policy to design a plan that would help those people above all else.
Because I think it is very, very important we call attention, particularly as conservatives, to the poor quality of coverage and care and access that low-income people get whether they are nominally uninsured or quote unquote insured under Medicaid.
And that’s I think something that I think you’re right that there is a degree to which conservatives see the low-income voters as not their voter. I think part of it is that there’s philosophical view that we shouldn’t just be handing money to people who didn’t earn it through work or something like that.
But I look at it differently. I say … you know, somebody asked me the other say, he said “Avik, is there a work requirement … ” (A conservative asked me this …) “Is there a work requirement in your plan for eligibility for these exchange subsidies for low-income people?” and I said no.
The guy said: “Well that’s a problem. We should have a work requirement.”
I said to him: “Would you ask for a work requirement for a low-income unemployed parent to send his child to primary school?” Of course he didn’t answer. And to me … that’s how I see health coverage. I see health coverage in exactly the same way which is … for the same reason we would want the child of the poor unemployed person to be able to go to a good school, we should want a child of the poor unemployed person to get access to good health care. I share that view that a lot of progressive share and what I contest is that Medicaid program is the vehicle with which to do it.
A call for bipartisanship
Harold: I’ve spent a long time working with low-income people, many of whom on Medicaid. I share your concerns that Medicaid has problems as a program, but I can tell you the overwhelming majority of people on Medicaid are very grateful to have it. This gentleman in South Carolina would have been very happy to have it. The people in Oregon are very happy to have it. If you can compare the satisfaction of people on Medicaid with the satisfaction of people on private insurance who are similar, Medicaid does very well. I agree with you it has a lot of problems. But I think that it is a very bad argument against universal coverage to point to the defects of Medicaid and I do think …
I hope that when Republicans read your plan, that one of the things that they take from it is … We have to find a way to get everybody covered. We have to do it in a way that is consistent with our principles … and I think Democrats and Republicans have to compromise on that because neither one of us can … We can’t do it alone … either side.
Avik: That is what I think my role is as a think tank guy. I think if you are even a reform oriented politician whether you are a Democrat or a Republican it is very hard for you to come up with a bi-partisan proposal because you are going to get attacked by your constituencies, both activists and primary voters for doing so. I think some guys have tried it; some guys like Ron Wyden have tried on the Democratic side.
I think guys like Paul Ryan and Tom Coburn have on the Republican side come up with bipartisan proposals, Joe Lieberman. And again these are people who people on the hard left and the hard right that might not like. I think my role as a think tank guy is to really flesh it out because nobody, thankfully, can primary challenge me … or at least I suppose they can try … but that is a strength of being in the academic or think tank world. I see it as our job to try to bridge some of those gaps and offer credible alternatives to the polarized environment we find ourselves.
Harold: This is probably a good place to stop. Thank you for devoting a large chunk of your afternoon to talking with me. Perhaps we should have had more vituperative argument to establish each of our credibility with our respective sides.
Avik: You tried.
Harold: I did. People would just have to take my word for it that you are conservative and I’m a liberal. I think this has been a fruitful conversation and I really appreciate it, and I wish you the best of luck.
Avik: Thanks Harold, I really enjoyed the challenging questions.
Harold Pollack is the Helen Ross Professor at the School of Social Service Administration. He is also Co-Director of The University of Chicago Crime Lab. He has published widely at the interface between poverty policy and public health. Pollack serves as a Fellow at the MacLean Center for Clinical Ethics at the University of Chicago, and as an Adjunct Fellow at the Century Foundation.
