






While his language was rather … impolitic, Bill Clinton told a hard truth about Obamacare this past Monday: This year’s sharp premium hikes will bring hardship to many of the roughly 9 million people who buy their health insurance in the individual market without benefit of a premium subsidy. He made a couple* of mistakes, though, and one of them cast light on an interesting part of his political id – and also gave a glimmer of an alternative path for the ACA.
With respect to those who earn too much to qualify for subsidies, the aspiring First Husband said:
The [private for-profit] insurance model doesn’t work here; it’s not like life insurance, it’s not like casualties, it’s not like predicting flooding. It doesn’t work. So Hillary believes we should simply let people who are above the line for getting these subsidies have access to affordable entry into the Medicare and Medicaid programs. They’ll all be covered, it will not hurt the program, we will not lose a lot of money. And we ought to do it.
While Hillary has thrown a Medicare buy-in option for people aged 55-64 into her potpourri of proposed ACA enhancements, she has not proposed a new initiative for letting “people who are above the line” for ACA premium subsidies buy into Medicaid – and neither has anyone else, as far as I know.**
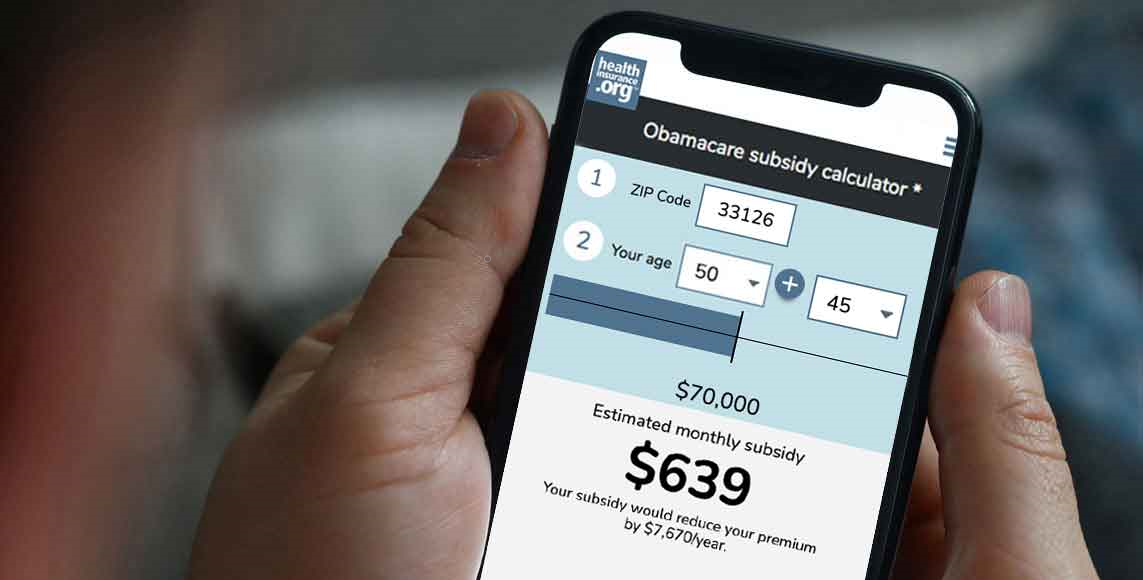
Generally, people earning too much to qualify for subsidies – that is, over 400 percent of the federal poverty level ($47,520 for an individual and $97,200 for a family of four) – would probably find Medicaid an unattractive option – first, because it’s stigmatized as “poor people’s insurance,” and more substantively, because the network of doctors and hospitals to which it provides access is often extremely limited. On the other hand, even relatively affluent people paying, say, $600 per month apiece for high-deductible private market insurance might find Medicaid’s comprehensive coverage and low copays at an affordable cost a welcome relief.
Medicaid-plus?
A Medicaid buy-in for anyone who needs it would be a huge mental leap in almost any imaginable American political context. There is, however, a kind of transitional object, created by the ACA, that a liberally inclined state could use to offer something very like it. That object is the Basic Health Program (BHP) that the ACA empowers states to establish for people at the lower range of subsidy eligibility in the ACA private plan marketplace – that is, for people whose household incomes are between 138 percent of the Federal Poverty Level (the cutoff for Medicaid eligibility) and 200 percent FPL. Legally present noncitizens with incomes below 138 percent FPL who are time-barred from Medicaid are also eligible for the BHP.
A BHP must offer coverage at least as comprehensive as a benchmark Silver plan, and with a premium no higher than the benchmark at the enrollee’s income level. That means that the actuarial value of the plans on offer must be at least 94 percent for enrollees with incomes up to 150 percent FPL, and at least 87 percent for those in the 150-200 percent FPL range. The maximum premium would be $125, the price of a benchmark Silver plan for a person with an income of 200 percent FPL ($23,760).
In practice, the two states that have implemented BHPs, Minnesota and New York, offer much lower premiums and out-of-pocket costs in the BHP than enrollees would find in the marketplace, New York’s BHP, the Essential Plan, has a $0 premium for enrollees with incomes up to 150 percent FPL and a $20 premium for those in the 150-200 percent FPL range. Their are no deductibles and no copays for those under 150 percent FPL, and an extremely low fee schedule for higher income enrollees. In Minnesota’s BHP, MinnesotaCare – adapted from a public insurance program pre-existing the ACA – premiums top out at $80 per month. The deductible is just $2.95 per month, and co-pays here too are low – e.g., $50 for an emergency room visit, and $15 for a physician visit.
More to Bill Clinton’s (inadvertent) point: the BHPs are structured like Medicaid managed care programs. That is, insurers, acting as managed care organizations (MCOs), contract directly with the state, and are paid rates comparable to or modestly above those paid to Medicaid MCOs. (In New York, Essential Plan insurers are paid 20 percent above Medicaid rates.) Enrollees generally have a choice from among at least three participating insurers.
Beyond the BHP?
Any state can start a BHP. The federal government will fund it by paying 95 percent of what it would have cost to subsidize BHP-eligible enrollees in the ACA marketplace. Obviously, a BHP does not solve the problem of soaring costs for those who earn too much to qualify for marketplace subsidies. It could, however, provide a stepping stone to a solution for that group. That’s because the ACA also empowers states to apply for innovation waivers to design alternatives to the basic ACA structure, provided that those alternatives offer equally comprehensive coverage to those eligible for ACA benefits, and at comparable cost. Thus a state could propose, via innovation waiver, to allow anyone who lacked access to employer-sponsored insurance or another public program (such as Medicaid or disability Medicare) to buy into the BHP.
The current premium spike in the ACA marketplace, averaging about 25 percent nationwide, ironically creates a great “buying opportunity” for many states if they want to start a BHP. The estimated cost of covering all enrollees would be based on 2017 premiums – a considerably bigger pot than was available in prior years (though the increase would vary widely by state). A more comprehensive program submitted via innovation waiver, to replace the ACA marketplace with a public program open to all who would have been eligible for marketplace coverage, would be funded at 100 percent of estimated marketplace cost at whatever premium levels are current when the waiver application is submitted.
A BHP that was open to all income levels would be a public option on steroids, as multiple insurers would participate. It would be in effect an all-public marketplace, or rather a public-private marketplace, with the state directly paying private insurers on a per-enrollee basis. That’s hardly a novel structure: it’s how managed Medicaid programs work, and also Medicare Advantage plans. The outlier in government-subsidized health insurance markets is actually the ACA marketplace, where insurers are left to free-form negotiate the rates they pay to healthcare providers, rather than paying rates tied to a government benchmark (Medicaid or Medicare).
Establishing a BHP marketplace open to all income levels would be disruptive: it might severely stress or kill off entirely the state’s existing individual market. But the insurers in that market could participate, as most New York insurers now participate in the state BHP. And to date, two states have considered or are now considering a more radical plan: a single payer system for the entire state, including the employer market. That would disrupt private insurers’ core business (employer-sponsored insurance) and require major tax increases. A public-private marketplace would disrupt only the relatively small individual market, which currently serves about 6 percent of the U.S. population.
Has Bill Clinton actively contemplated a Medicaid buy-in, or was his suggestion just a slip of the tongue? He did state outright that the individual market does not, cannot work for the unsubsidized. The Medicare buy-in proposed by Hillary would cover only a slice of that market, perhaps 25 percent. There’s no knowing the Big Dog’s thought process. But he did let slip an original idea worth mulling.
* Charles Gaba fingers another Bill Clinton error here.
** Update: States do run Medicaid and CHIP buy-in programs for certain classes of children (often those with disabilities) in households with incomes exceeding Medicaid or CHIP eligibility standards, and for adults with disabilities who want to continue working. But there are no buy-in programs for able-bodied adults with incomes that disqualify them for ACA subsidies. (Language in the paragraph linked to this note has been edited for clarity.)
Andrew Sprung is a freelance writer who blogs about politics and policy, particularly health care policy, at xpostfactoid. His articles about the rollout of the Affordable Care Act have appeared in The Atlantic and The New Republic. He is the winner of the National Institute of Health Care Management’s 2016 Digital Media Award.
