Medicaid eligibility and enrollment in Minnesota
Medicaid expansion plus MinnesotaCare = coverage up to 200% FPL


Who is eligible for Medicaid in Minnesota?
In addition to aged, blind, and disabled people with limited financial means, residents who meet the following requirements are eligible for Medical Assistance, which is the name of Minnesota’s Medicaid program:1 (Note that the following eligibility limits include a built-in 5% income disregard that’s used for Medicaid eligibility determination for these populations.)2
- Adults with household incomes up to 138% of poverty (adults with incomes above 138% of poverty but not more than 200% of poverty are eligible for coverage under MinnesotaCare,3 which is the state’s Basic Health Program).
- Pregnant women with household incomes up to 283% of poverty (coverage for the mother continues for 12 months after the baby is born)4
- Children 0-2 in households with income up to 288% of poverty.
- Children from 2-18 in households with income up to 280% of poverty.
See current dollar amounts for the income limits for each eligibility category.
for 2026 coverage
0.0%
of Federal Poverty Level
Apply for Medicaid in Minnesota
Enroll online at MNsure. Call 1-855-366-7873 for help enrolling. Enroll in person at your County Human Services office.
Eligibility: Children up to 1 year with household income up to 283% of FPL. Children ages 1-18 with household income up to 275% of FPL. Pregnant women with household income up to 278% of FPL. Adults with household income up to 138% of FPL; adults with income between 138% and 200% of FPL qualify for MNCare.



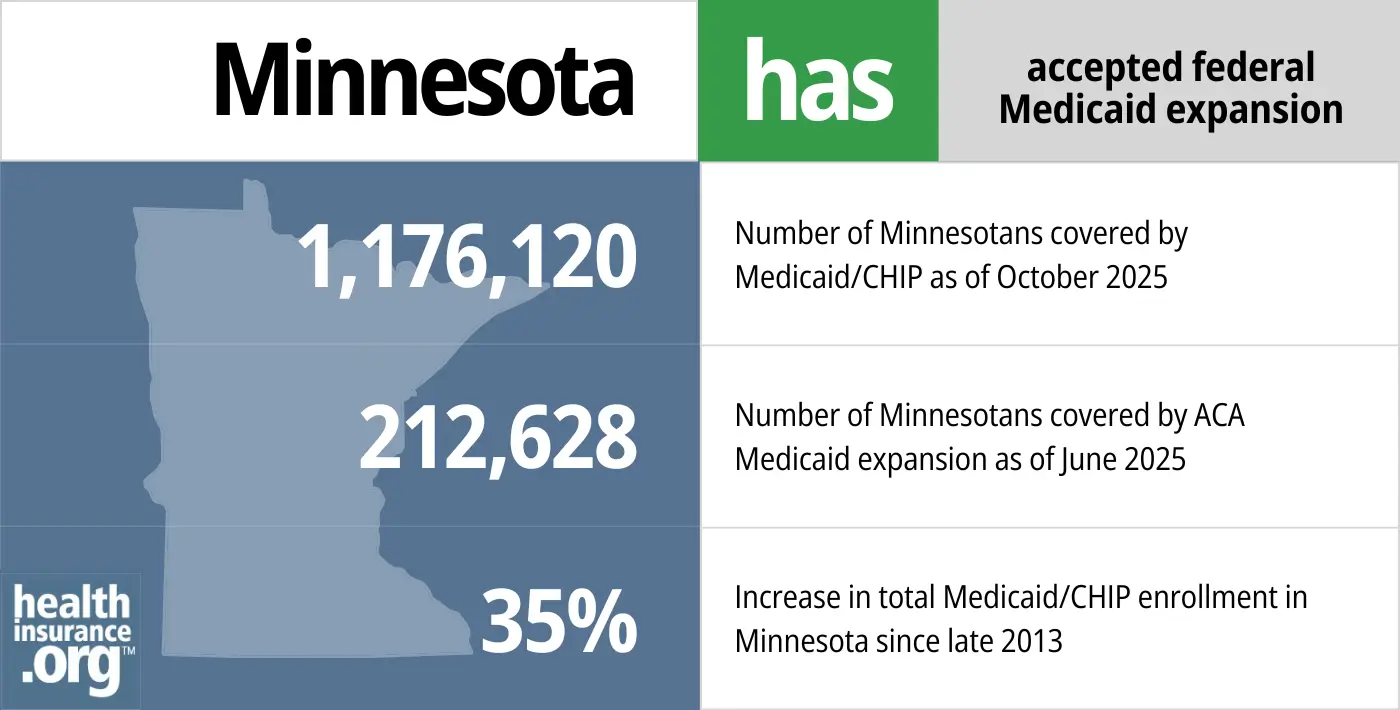
Has Minnesota implemented Medicaid expansion?
Minnesota expanded Medicaid as called for in the ACA, starting in 2014.5 This allows low-income adults (under the age of 65) to enroll in Medicaid, even if they’re not disabled, pregnant, or the parent of a minor child. The federal government pays 90% of the cost of covering the Medicaid expansion population, while the state covers the other 10%.
Starting in 2027, there will be a work requirement for Medicaid expansion, and eligibility for this population will be redetermined twice per year, instead of once per year. These changes are a result of the federal “One Big Beautiful Bill” that was enacted in 2027.6
As of mid-2025, more than 212,000 Minnesota residents were enrolled in expanded Medicaid. Total Medicaid/CHIP enrollment in Minnesota, including the expansion population, stood at more than 1.1 million at that point.7
Minnesota’s Medicaid enrollment in early 2026 was 30% higher than it had been in the fall of 2013.8 That growth is due primarily to Medicaid expansion. It had been even higher during the COVID pandemic, when disenrollments were paused for three years. But eligibility was redetermined for all enrollees in 2023 and 2024, and many people were disenrolled (details below).
- 1,135,076 – Number of Minnesotans covered by Medicaid/CHIP as of February 20269
- 212,628 – Number of Minnesotans covered by ACA Medicaid expansion as of June 202510
- 33%– Increase in total Medicaid/CHIP enrollment in Minnesota since late 20138
Explore our other comprehensive guides to coverage in Minnesota

The ACA Marketplace allows individuals and families to shop for and enroll in ACA-compliant health insurance plans. Subsidies may be available based on household income to help lower costs.
Hoping to improve your smile? Dental insurance may be a smart addition to your health coverage. Our guide explores dental coverage options in Minnesota.

Use our guide to learn about Medicare, Medicare Advantage, and Medigap coverage available in Minnesota as well as the state’s Medicare supplement (Medigap) regulations.

Short-term health plans provide temporary health insurance for consumers who may find themselves without comprehensive coverage.
Frequently asked questions about Minnesota Medicaid eligibility and enrollment
How do I enroll in Medicaid in Minnesota?
If you’re under 65 and not on Medicare:
- You can enroll in Medical Assistance (Minnesota Medicaid) online at MNsure, the state-run health insurance exchange (if the system determines that you’re eligible for Medical Assistance, your enrollment will be managed by the Minnesota Department of Human Services).11
- You can call 855-366-7873 for help enrolling or to locate a navigator in your area who can assist you with the enrollment process in person.
- You can enroll in person at your County Human Services office (including Tribal Health Care offices).
If you are 65 or older or have Medicare, visit one of these websites (seniors and people with disabilities) for help applying for Medicaid.
How does Medicaid assist Medicare beneficiaries in Minnesota?
Many Medicare beneficiaries receive assistance through Medicaid with the cost of Medicare premiums, co-pays, deductibles, and services not covered by Medicare — such as long-term care.
Our guide to financial assistance for Medicare beneficiaries in Minnesota explains these benefits, including Medicare Savings Programs, Extra Help, long-term care coverage, and income guidelines for assistance.
How many people were disenrolled from Minnesota Medicaid after the pandemic?
During the COVID pandemic, from March 2020 through March 2023, Medicaid disenrollments were paused nationwide. But that rule ended March 31, 2023. Medicaid disenrollments resumed in Minnesota in July 2023, and 439,480 Minnesota residents were disenrolled from Medicaid during the year-long “unwinding” of the pandemic-era continuous coverage rule.12
People with MinnesotaCare (the state’s Basic Health Program, discussed in more detail below) received their renewal notices in October 2023, for coverage effective in January 2024.13
People who were no longer eligible for Medicaid may have found that they’re eligible for MinnesotaCare instead. And people who aren’t eligible for either program are likely to be eligible for either an employer’s health plan or a subsidized policy through MNsure, the state-run exchange.
CMS reported that 14,510 people transitioned from Minnesota Medicaid to a private plan in the Marketplace (MNsure) during the unwinding process, and another 9,238 people transitioned from Minnesota Medicaid to MinnesotaCare.14
Minnesota enacted SF2265 in 2023, which ensured that for Medical Assistance enrollees who are subject to asset tests, including those age 65 and older, assets were disregarded during their first renewal after the pandemic-era continuous coverage period, and would not be taken into consideration until their second annual renewal.15
SF2265 initially included various other provisions designed to ease the transition from the pandemic-era continuous coverage rule, including additional state-funded cost-sharing reductions for MNsure plans, and continuous coverage Medicaid rules for children under the age of six. But those provisions were not included in the version of the bill that was enacted.15
Minnesota Medicaid history and details
Minnesota Medicaid estate recovery is now limited to cases in which long-term care was provided
Minnesota’s Medicaid program has utilized estate recovery (required under state and federal law) since 1967 as a means of recouping Medicaid costs after an enrollee dies. The estate recovery program applies to people who were 55 or older at the time they incurred Medicaid claims, and the program allowed the state to place liens against the enrollees’ estates, so that some or all of the money would be paid back to the state.
Before the ACA, the vast majority of adults 55 or older who were covered by Medicaid were elderly, low-income residents who needed long-term care (Medicare does not cover long-term care, but Medicaid does if the person’s income and assets are low enough). But starting in 2014, large numbers of residents — many of whom were 55 or older — became eligible for Medicaid, and many were caught off-guard when they found out that liens were being filed against their estates.
Minnesota lawmakers addressed the issue in 2016, amending the state’s existing protocol for Medicaid estate recovery. The state announced that pending federal approval, Medicaid estate recovery in Minnesota would be limited to cases in which long-term care was covered. The state intended to make that change retroactive to January 2014, but CMS did not approve that.16 Instead, the new rules, which limit estate recovery to long-term care costs, apply to estate claims that were pending as of July 1, 2016, and to the estates of people who die after July 1, 2016.17
Minnesota Care available up to 200% of poverty
In addition to Minnesota Medicaid, the state provides MinnesotaCare (MNCare) for residents with incomes above 138% of poverty, up to 200% of poverty. MinnesotaCare is a Basic Health Program (as described below, the program pre-dates the ACA, but transitioned to an ACA Basic Health Program in 2015).
As of May 2026, there were 87,391 people enrolled in MinnesotaCare.18
Unlike Minnesota’s Medicaid program, MNCare has a monthly premium that ranges as high as $80 in 2026. The premium is calculated on a sliding scale and people on the lower end of the income scale pay less than $10/month — in some cases, $0.19
From 2021 through 2025, while federal subsidy enhancements were in place, MinnesotaCare premiums were eliminated for many enrollees, and only ranged as high as $28/month for those on the higher end of the MinnesotaCare income scale. But the premiums had been as high as $80/month before the American Rescue Plan increased federal health insurance subsidies, and that’s once again the case in 2026,20 after Congress let the federal subsidy enhancements expire.
Unsurprisingly, MinnesotaCare enrollment dropped in 2026, after the higher premiums took effect: 106,204 people had been enrolled in December 2025, and that dropped to 78,540 in January 2026 (although as noted above, it had grown to 87,391 by May 2026).21
(Basic Health Program funding is based on the state receiving 95% of the money that the federal government would otherwise have spent on Marketplace subsidies for the people who end up being eligible for the BHP. Because federal subsidy funding dropped in 2025 after the subsidy enhancements expired, BHPs are receiving less federal funding in 2026, which is why MinnesotaCare premiums increased.)
The preferred enrollment method for MinnesotaCare is through MNsure, and enrollment in Minnesota Medicaid and MinnesotaCare is open year-round.
As noted above, disenrollments for MinnesotaCare were paused during the pandemic, just like disenrollments for Medicaid. But MinnesotaCare renewals (and disenrollments) resumed in October 2023, for coverage effective in 2024.13
MNCare has existed in Minnesota since 1992, but it became a much more robust program in 2014. As of January 2015, MinnesotaCare transitioned to a Basic Health Program under the ACA. BHPs are a provision of the ACA that any state can implement, but Minnesota was the only state to do so in 2015. New York established a BHP, effective January 2016 (NY temporarily shifted its BHP to a different type of program, with a higher income limit, in mid-2024, but plans to shift it back to a BHP in mid-2026). Oregon implemented a BHP in mid-2024, and DC did so in 2026.
Numerous improvements were made to MNCare effective January 1, 2014. The program no longer has a $1,000 copay for hospitalization, or a $10,000 cap on inpatient benefits. The asset test has been eliminated just as it was for Medicaid, and premiums have been significantly reduced. It used to be available only to applicants who had been uninsured for at least four months, but that provision was eliminated in 2014.
Minnesota Medicaid enrollment
In the fall of 2013, prior to the launch of the ACA’s exchanges, Minnesota’s total Medicaid/CHIP enrollment stood at 873,040.
As of early 2026, there were a total of 1,135,076 people enrolled in Medicaid/CHIP in Minnesota.22
Most of these enrollees are enrolled in managed care programs,23 which means the state contracts with a private health insurer to administer the benefits.
Minnesota Medicaid history
Minnesota was one of the six states that enacted Medicaid as soon as the program became available, in January 1966.
Minnesota had some of the country’s most generous eligibility guidelines for Medicaid before expansion under the ACA (up to 100% of poverty for adults with dependent children, and up to 75% of poverty for those without dependent children). The state also became the first in the nation to establish a Basic Health Program under the ACA.

Looking for more information about other options in your state?
Need help navigating health insurance options in Minnesota?
Explore more resources for options in MN including ACA coverage, short-term health insurance, dental and Medicare.
Speak to a sales agent at a licensed insurance agency.
Footnotes
- ”Medicaid, Children’s Health Insurance Program, & Basic Health Program Eligibility Levels” Centers for Medicare and Medicaid Services. December 2023. Accessed Sep. 30, 2025 ⤶
- ”With respect to MAGI conversion, how will the 5% disregard be applied?” Centers for Medicare & Medicaid Services. Accessed Sep. 30, 2025 ⤶
- ”MinnesotaCare” Minnesota Department of Human Services. Accessed Sep. 30, 2025 ⤶
- ”Medicaid Postpartum Coverage Extension Tracker” KFF.org. Mar. 19, 2026 ⤶
- ”Minnesota HF 9” BillTrack50. Enacted Feb. 21, 2013 ⤶
- ”What the new federal budget law means for Medicaid” MN.gov. Accessed June 2, 2026 ⤶
- ”Medicaid Enrollment – New Adult Group” (See quarterly enrollment updates for latest numbers) Centers for Medicare & Medicaid Services. Data as of June 2025. Accessed June 2, 2026 ⤶
- Total Monthly Medicaid & CHIP Enrollment and Pre-ACA Enrollment, KFF.org, Accessed June 2, 2026 ⤶ ⤶
- ”October 2025 Medicaid & CHIP Enrollment Data Highlights” Medicaid.gov, Accessed February 2026 ⤶
- ”Medicaid Enrollment – New Adult Group” Centers for Medicare & Medicaid Services. Accessed February 2026 ⤶
- General FAQs about MNsure. MNsure. Accessed June 2, 2026 ⤶
- ”Medicaid Enrollment and Unwinding Tracker” (State Data, Minnesota). KFF.org. Sep. 4, 2025 ⤶
- Minnesota Health Care Programs: Plan to unwind continuous eligibility coverage. Minnesota Department of Human Services. January 2023. ⤶ ⤶
- State-based Marketplace (SBM) Medicaid Unwinding Report. Centers for Medicare and Medicaid Services. Accessed Sep. 30, 2025; Data through September 2024 ⤶
- Minnesota Senate File 2265, enacted March 2023. BillTrack50. ⤶ ⤶
- ”DHS Explains: Changes to MA Estate Recovery Resulting from CMS Approval of a Revised State Plan Amendment; and a New Statewide Funeral Expenses Policy” Minnesota Department of Human Services. Accessed Sep. 30, 2025 ⤶
- ”Minnesota Health Care Programs. Timeline of Medical Assistance Estate Recovery” Minnesota Department of Human Services. Accessed Sep. 30, 2025 ⤶
- ”Managed Care Enrollment Figures” Minnesota Department of Human Services. Data through May 2026. Accessed June 2, 2026 ⤶
- ”How much does it cost?” Minnesota Department of Human Services. Accessed Sep. 30, 2025 ⤶
- ”MinnesotaCare Premium Estimator Table, Effective January 1, 2026 – December 31, 2026” Minnesota Department of Human Services. Accessed Sep. 30, 2025 ⤶
- ”Managed Care Enrollment Figures” Minnesota Department of Human Services. Data for December 2025, January 2026, and May 2026. Accessed June 2, 2026 ⤶
- ”Total Monthly Medicaid & CHIP Enrollment and Pre-ACA Enrollment” KFF.org, Accessed June 2, 2026 ⤶
- ”Managed care enrollment figures” Minnesota Department of Human Services. Accessed Sep. 30, 2025 ⤶

