Find North Carolina Health Insurance Marketplace Coverage for 2026

Compare ACA plans and check subsidy savings from a licensed third-party health insurance agency.
North Carolina Health Insurance Marketplace Guide
This guide, including the FAQs below, was developed to help you understand the health insurance options and possible financial assistance available to you and your family in North Carolina.
The health plan options found in North Carolina’s ACA Marketplace/exchange are designed to cover people who don’t have access to Medicare, Medicaid, or an employer’s health plan. North Carolina uses the federally facilitated health insurance exchange platform — Healthcare.gov — for residents to purchase its ACA Marketplace plans.
North Carolina’s Marketplace provides access to health insurance products from six private insurers for 2026,1 down from nine in 2025 (see below for details about carrier exits and premium changes for 2026).
The federal government helps pay for insurance through an advance premium tax credit (APTC) if you buy coverage from the exchange and are eligible for the tax credit based on your income. Some enrollees are also eligible for cost-sharing reductions, which reduce out-of-pocket costs on Silver-level plans for eligible enrollees.
Although the majority of North Carolina Marketplace enrollees still qualify for subsidies in 2026, some people lost their subsidies at the end of 2025 due to the expiration of federal subsidy enhancements. And although the average subsidy amount in 2026 is larger than it was in 2025 (due to increases in full-price premiums), the subsidies are smaller than they would have been if the subsidy enhancements had been extended (see details below).
North Carolina Medicaid expansion took effect on December 1, 2023, making hundreds of thousands of North Carolina residents newly eligible for Medicaid. Some were previously in the coverage gap, while others were previously eligible for subsidies to offset the cost of Marketplace coverage.2
*Values displayed by this tool are from data generated by CMS and reflect 2026 Marketplace health plans purchased in each state. The values returned are averages based on the plans purchased by consumers of each selected state: subsidy and premium values vary based on factors such as zip code, age, household size, and income.
North Carolina Marketplace quick facts
Frequently asked questions about health insurance in North Carolina
Who can buy Marketplace health insurance in North Carolina?
To qualify for health coverage through the North Carolina Marketplace, you must:5
- Live in North Carolina
- Be lawfully present in the United States
- Not be incarcerated
- Not be enrolled in Medicare
Eligibility for financial assistance (premium subsidies and cost-sharing reductions) depends on your income and how it compares with the cost of the second-lowest-cost Silver plan in your area – which depends on your age and location. In addition, to qualify for financial assistance with your Marketplace plan you must:
- Not have access to affordable health coverage through your employer. If your employer offers coverage but you feel it’s too expensive, you can use our Employer Health Plan Affordability Calculator to see if you might qualify for premium subsidies in the Marketplace.
- Not be eligible for Medicaid or CHIP.
- Not be eligible for premium-free Medicare Part A.6
- If married, file a joint tax return.7
- Not be able to be claimed by someone else as a tax dependent.7
When can I enroll in an ACA-compliant plan in North Carolina?
In North Carolina, the open enrollment period for 2026 individual/family health coverage ended on January 15, 2026.8
Starting in the fall of 2026, the open enrollment period will be shorter. In states like North Carolina that use HealthCare.gov as their Marketplace, the enrollment window will run from November 1 through December 15, and all policies selected during open enrollment will take effect January 1. This is due to a federal rule change that was finalized in 2025.
Outside of open enrollment, a qualifying event is generally necessary to enroll or make changes to your coverage, although American Indians and Alaska Natives can enroll year-round without a specific qualifying life event.
If you have questions about open enrollment, you can learn more in our comprehensive guide to open enrollment. We also have a comprehensive guide to special enrollment periods.
How do I enroll in a North Carolina Marketplace plan?
If you’re eligible for an ACA Marketplace plan, there are several ways you can enroll:
- Online through HealthCare.gov
- By phone at (800) 318-2596
- With local help in your community from an agent/broker, Navigator, or certified application counselors (these individuals are available to help you over the phone, online, and sometimes in-person, depending on your preference)
- Through an approved enhanced direct enrollment entity.9
How can I find affordable health insurance in North Carolina?
North Carolina uses the federally facilitated exchange for individual market plans, so residents who buy their own health insurance enroll through HealthCare.gov.
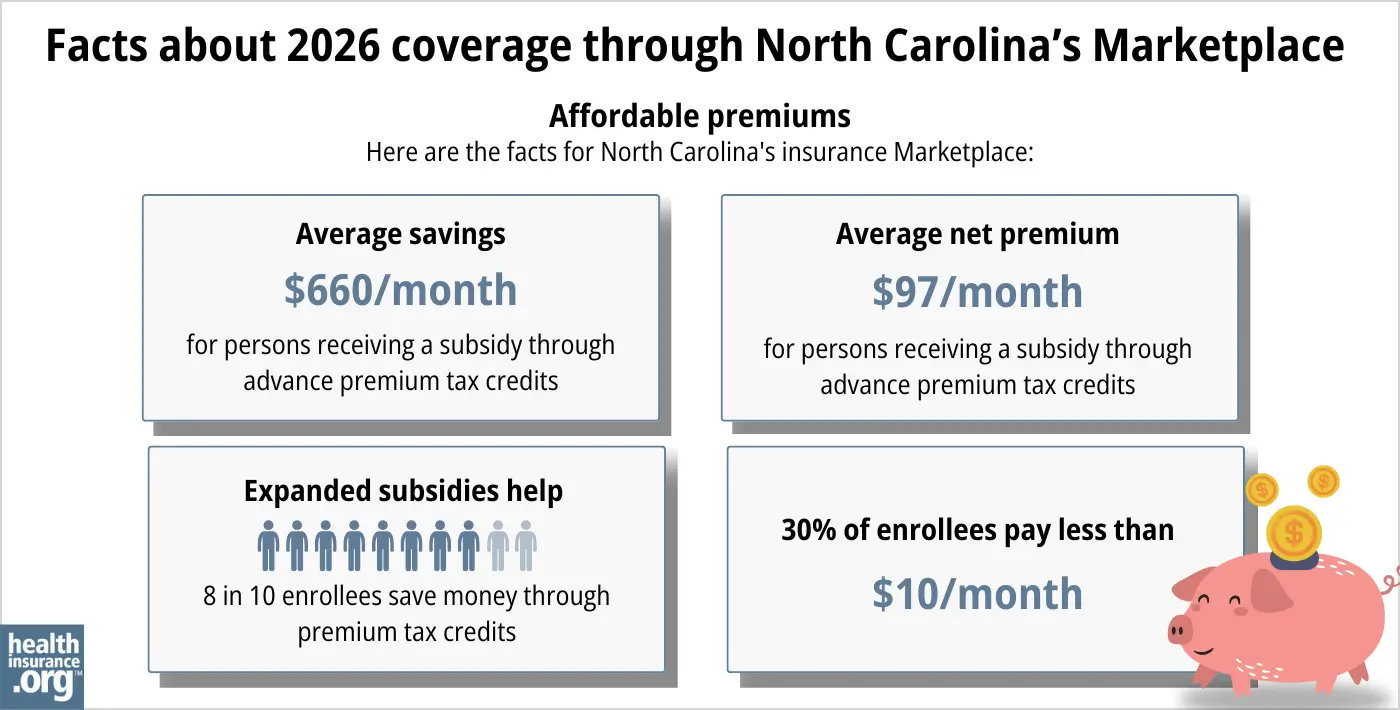
During the open enrollment period for 2026 coverage, 87% of the people who enrolled in Marketplace coverage in North Carolina were eligible for premium tax credits (subsidies) that averaged $660/month. After subsidies were applied, the average subsidy-eligible enrollee’s monthly cost was about $97/month (when we include those who paid full price, the average net premium was $180/month).10
Although most North Carolina Marketplace enrollees qualify for premium tax credits in 2026, the tax credits cover a smaller share of enrollees’ total premiums in 2026, and are available to fewer people, due to the expiration of federal subsidy enhancements at the end of 2025. Premium tax credits were used by 94% of North Carolina Marketplace enrollees in 2025. And the average net premium in 2025 (including those who paid full price) was $97/month.11 So the expiration of subsidy enhancements resulted in an 85% increase in average net premiums in 2026, despite the fact that many people downgraded to lower-premium Bronze plans.12
Note: Average premium subsidies are larger in North Carolina in 2026 than they were in 2025: An average of $660/month in 2026,12 up from $573/month in 2025.11 But this is because the underlying premiums increased so much. If the subsidy enhancements had been extended, the subsidies would have been even larger for 2026. And although the average subsidy amount increased, it’s still covering a smaller share of enrollees’ total premiums.
Source: CMS.gov 10
In addition to premium tax credits, the ACA also provides cost-sharing reductions (CSR) to enrollees with household income up to 250% of the federal poverty level, as long as they purchase a Silver-level plan.13
Forty-five percent of North Carolina Marketplace enrollees were receiving CSR benefits in 2025,11 but that dropped to just 28% in 2026.12 To be clear, nothing changed about CSR benefits or eligibility. But a significant number of North Carolina Marketplace enrollees downgraded to lower-premium Bronze plans for 2026, and CSR benefits are forfeited if a person doesn’t enroll in a Silver plan. (45% of North Carolina Marketplace enrollees selected Bronze plans for 2025,11 and that increased to 64% for 2026.)12
Catastrophic plans are not available in the North Carolina Marketplace for 2026.14 But when they were available in 2025, only 106 people selected them.11
How many insurers offer Marketplace coverage in North Carolina?
Six insurers offer Marketplace plans in North Carolina for 2026, with coverage areas that vary from one insurer to another:1
- Ambetter/Centene
- AmeriHealth Caritas
- Blue Cross and Blue Shield of NC
- Cigna
- Oscar
- UnitedHealthcare
Nine insurance companies offered individual/family health plans through North Carolina’s Marketplace for 2025,15 but three of them left North Carolina’s individual market at the end of 2025.
Aetna, Celtic/WellCare, and CareSource exited the state’s market. According to their market withdrawal filings in SERFF, Aetna had about 130,000 enrollees in North Carolina who had to select new coverage for 2026. Celtic/WellCare had only 25 individual market enrollees in North Carolina, but they too, had to select new plans during open enrollment.16 HAP CareSource had about 3,000 enrollees,17 all of whom needed to pick new plans for 2026.18
Are Marketplace health insurance premiums increasing in North Carolina?
The following average rate changes were approved for 2026 for the insurers that offer individual/family plans in North Carolina’s health insurance Marketplace (calculated before subsidies are applied; after-subsidy increases were much more significant, as described below, because Congress did not extend the federal subsidy enhancements that expired at the end of 2025).
North Carolina’s ACA Marketplace Plan 2026 APPROVED Rate Increases by Insurance Company |
|
|---|---|
| Issuer | Percent Increase |
| Aetna Health Inc. | Exited market |
| Ambetter/Centene | 23.4% |
| AmeriHealth Caritas | 36.4% |
| Blue Cross and Blue Shield of NC | 29.4% |
| CareSource | Exited market |
| Celtic/WellCare | Exited market |
| Cigna | 27.5% |
| Oscar | 16.9% |
| UnitedHealthcare | 32.3% |
Source: North Carolina Department of Insurance1 Market exits based on SERFF Filings16 and carrier statements18
The weighted average rate increase for 2026 was almost 28% in North Carolina.17 These significant rate increases were driven in part by the expiration of the federal subsidy enhancements that had been in place since 2021, and by the Marketplace rules that were finalized by HHS in 2025. Both had the effect of reducing enrollment, which tends to drive premiums higher (the people who cancel their coverage tend to be healthy, so the overall risk pool becomes less healthy).
But average after-subsidy premium increases were much larger than 28%, because Congress did not extend the subsidy enhancements that expired at the end of 2025. The expiration of the subsidy enhancements resulted in:
- The return of the “subsidy cliff,” meaning subsidies are no longer available to anyone with a household income above 400% of the federal poverty level.
- Enrollees having to pay a larger percentage of their household income for their Marketplace coverage, as subsidies now cover a smaller share of the total premiums.
Here are some examples of the after-subsidy premium increases in Charlotte, North Carolina:19
- 40-year-old earning $40,000:
- Lowest-cost plan in 2025 was $31/month
- Lowest-cost plan in 2026 is $151/month
- 60-year-old earning $63,000:
- Lowest-cost plan in 2025 was $187/month
- Lowest-cost plan in 2026 is $949/month (due to the return of the subsidy cliff)
For perspective, here’s a summary of how average unsubsidized premiums have changed each year in North Carolina’s individual/family market:
- 2015: Average increase of 12%20
- 2016: Average increase of 28.1%21
- 2017: Average increase of 24.3%22
- 2018: Average increase of 14.8%23
- 2019: Average decrease of 3.9%24
- 2020: Average decrease of 5.6%25
- 2021: Average preliminary increase of 4%26
- 2022: Average increase of 3.2%27
- 2023: Average increase of 7.93%28
- 2024: Average decrease of 1.3%29
- 2025: Average increase of 7%15
How many people are insured through North Carolina’s Marketplace?
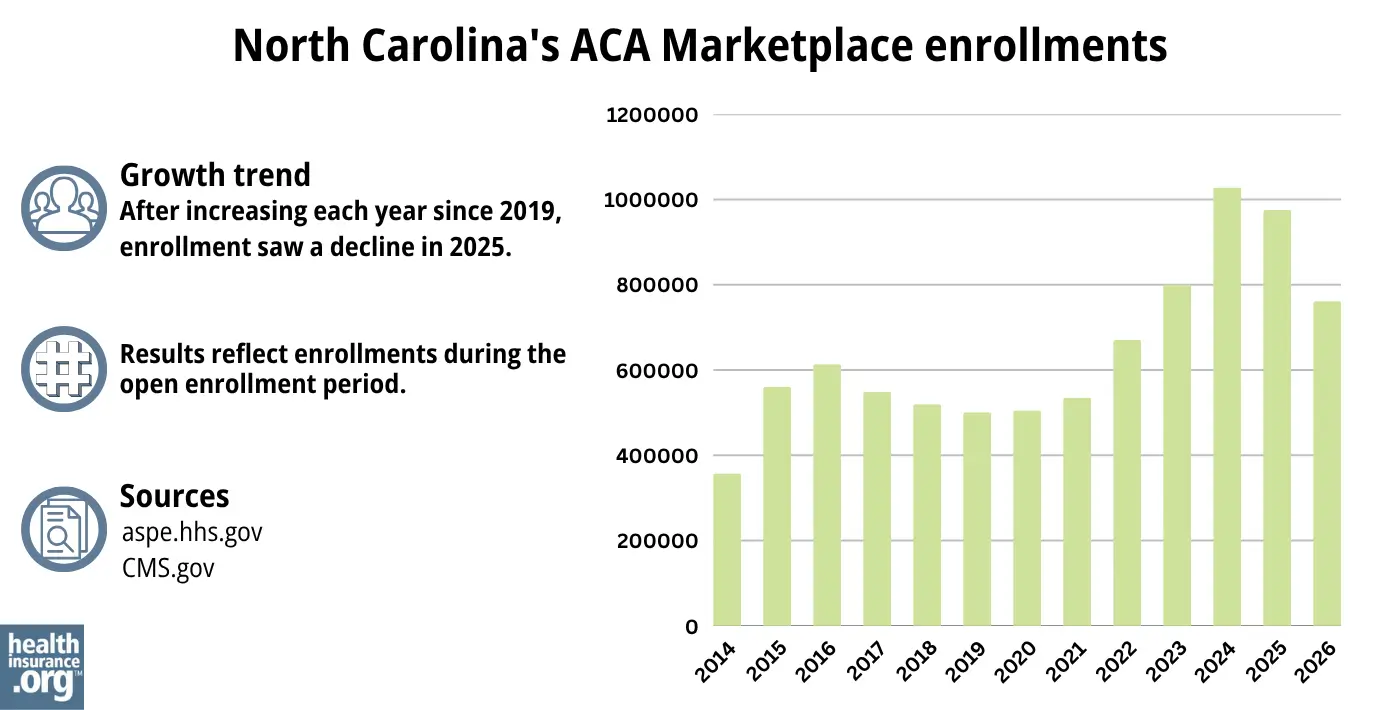
761,457 people selected plans through the North Carolina Marketplace during the open enrollment period for 2026 coverage.10
This was a drop of nearly 22% from the 975,110 people who had enrolled the year before, during the open enrollment period for 2025 coverage.30 The enrollment drop, which was the largest in the nation,31 happend largely because federal subsidy enhancements expired at the end of 2025, resulting in coverage becoming significantly more expensive in 2026.
Although most areas of the country reached record-high enrollment in 2025, that was not the case in North Carolina (see chart below). The record enrollment level in North Carolina came the year before, when 1,027,930 people enrolled during the open enrollment period for 2024 coverage.32
The record high enrollment for 2024 happened even though Medicaid expansion took effect in North Carolina in December 2023.
Before Medicaid expansion, people with income between 100% and 138% of the poverty level were eligible for Marketplace subsidies, whereas they’re now eligible for Medicaid instead. So states tend to see a dip in their Marketplace enrollment after expanding Medicaid. But North Carolina’s enrollment reached a significant new record high for 2024.
The increase in enrollment (which had been ongoing in North Carolina since 2021) was driven in part by the American Rescue Plan (ARP). Under the ARP, ACA’s premium subsidies were larger and more widely available. The ARP’s subsidy enhancements were extended through 2025 by the Inflation Reduction Act.33 But as noted above, these subsidy enhancements expired at the end of 2025, because Congress did not extend them again.
The enrollment increase in 2024 was also due to the “unwinding” of the pandemic-era Medicaid continuous coverage rule. Between June 2023 and April 2024, more than 272,000 people in North Carolina were disenrolled from Medicaid and transitioned to a Marketplace plan.34
Source: 2014,35 2015,36 2016,37 2017,38 2018,39 2019,40 2020,41 2021,42 2022,43 202344 2023,45 2024,46 202530 202610
What health insurance resources are available to North Carolina residents?
HealthCare.gov
800-318-2596
State Exchange Profile: North Carolina
The Henry J. Kaiser Family Foundation overview of North Carolina’s progress toward creating a state health insurance exchange.
North Carolina Institute of Medicine (NCIOM)
Health Insurance Smart NC
Assists people insured by private health plans, Medicaid, or other plans in resolving problems pertaining to their health coverage; assists uninsured residents with access to care.
Toll free: 1-877-885-0231
Managed Care Patient Assistance Program
Serves consumers who are members of managed health benefit plans.
(919) 733-6272 / Toll-Free: 1-866-867-6272 (in North Carolina only)
[email protected]
Community Care of North Carolina
Legal Aid of North Carolina (855-733-3711)

Looking for more information about other options in your state?
Need help navigating health insurance options in North carolina?
Explore more resources for options in NC including short-term health insurance, dental, Medicaid and Medicare.
Speak to a sales agent at a licensed insurance agency.
Footnotes
- ”2026 Plan Year ACA Rate Filings” North Carolina Department of Insurance – Life & Health Division. Accessed Nov. 2, 2025 ⤶ ⤶ ⤶
- Questions and Answers about Medicaid Expansion. North Carolina Medicaid Division of Health Benefits. Accessed November 2023. ⤶
- ”2026 OEP State-Level Public Use File (ZIP)” Centers for Medicare & Medicaid Services, Accessed July 9, 2026 ⤶ ⤶
- ”2026 Plan Year ACA Rate Filings” North Carolina Department of Insurance – Life & Health Division. July 31, 2025 *The above is based on the most current data available. ⤶
- ”A quick guide to the Health Insurance Marketplace” HealthCare.gov ⤶
- Medicare and the Marketplace, Master FAQ. Centers for Medicare and Medicaid Services. Accessed Mar. 22, 2026 ⤶
- Premium Tax Credit — The Basics. Internal Revenue Service. Accessed Mar. 22, 2026 ⤶ ⤶
- “When can you get health insurance?” HealthCare.gov, 2023 ⤶
- “Entities Approved to Use Enhanced Direct Enrollment” CMS.gov, Dec. 8, 2025 ⤶
- ”2026 Marketplace Open Enrollment Period Public Use Files” CMS.gov. April 2026 ⤶ ⤶ ⤶ ⤶
- ”2025 Marketplace Open Enrollment Period Public Use Files” Centers for Medicare & Medicaid Services. Accessed May 5, 2026 ⤶ ⤶ ⤶ ⤶ ⤶
- ”2026 Marketplace Open Enrollment Period Public Use Files” Centers for Medicare & Medicaid Services. Accessed May 5, 2026 ⤶ ⤶ ⤶ ⤶
- ”APTC and CSR Basics” Centers for Medicare & Medicaid Services. June 2024. ⤶
- ”Policy Changes Bring Renewed Focus on High-Deductible Health Plans” KFF.org. Jan. 5, 2026 ⤶
- ”North Carolina: *Final* avg. unsubsidized 2025 #ACA rate changes: +7.0% (updated)” ACA Signups. Oct. 29, 2024 ⤶ ⤶
- ”SERFF tracking number CELT-134533905 and AETN-134525406″ North Carolina SERFF Filings. Accessed Aug. 12, 2025 ⤶ ⤶
- ”2026 FINAL Gross Rate Changes – North Carolina: +27.7%; what happened to ~263,000 “missing” enrollees?? (updated)” ACA Signups. Nov. 1, 2025 ⤶ ⤶
- ”General Plan Information” CareSource. Accessed Nov. 2, 2025 ⤶ ⤶
- ”See Plans & Prices” (zip 28105) HealthCare.gov Accessed Nov. 2, 2025 ⤶
- Analysis Finds No Nationwide Increase in Health Insurance Marketplace Premiums. The Commonwealth Fund. December 2014. ⤶
- FINAL PROJECTION: 2016 Weighted Avg. Rate Increases: 12-13% Nationally* ACA Signups. October 2015. ⤶
- Avg. UNSUBSIDIZED Indy Mkt Rate Hikes: 25% (49 States + DC). ACA Signups. August 2016. ⤶
- 2018 Rate Hikes. ACA Signups. October 2017 ⤶
- 2019 Rate Hikes. ACA Signups. October 2018. ⤶
- 2020 Rate Changes. ACA Signups. October 2019. ⤶
- 2021 Rate Changes. ACA Signups. October 2020. ⤶
- 2022 Rate Changes. ACA Signups. October 2021. ⤶
- UPDATED: FINAL Unsubsidized 2023 Premiums: +6.2% Across All 50 States +DC. ACA Signups. Accessed November 2023. ⤶
- North Carolina: *Final* Avg. Unsubsidized 2024 #ACA Rate Changes: -1.3% (Updated). ACASignups.net, October 2023 ⤶
- “2025 Marketplace Open Enrollment Period Public Use Files” CMS.gov, May 2025 ⤶ ⤶
- ”2026 Rate Change Project” ACA Signups. Oct. 3, 2025 ⤶
- ”Health Insurance Marketplaces 2024 Open Enrollment Period Report” CMS.gov. March 22, 2024 ⤶
- “Health Insurance Marketplaces 2023 Open Enrollment Report” CMS.gov, Accessed August 2023 ⤶
- HealthCare.gov Marketplace Medicaid Unwinding Report. Medicaid.gov. Data through April 2024; Accessed Aug. 15, 2024 ⤶
- “ASPE Issue Brief (2014)” ASPE, 2015 ⤶
- “Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report”, HHS.gov, 2015 ⤶
- “HEALTH INSURANCE MARKETPLACES 2016 OPEN ENROLLMENT PERIOD: FINAL ENROLLMENT REPORT” HHS.gov, 2016 ⤶
- “2017 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2017 ⤶
- “2018 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2018 ⤶
- “2019 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2019 ⤶
- “2020 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2020 ⤶
- “2021 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2021 ⤶
- “2022 Marketplace Open Enrollment Period Public Use Files” CMS.gov, 2022 ⤶
- “Health Insurance Marketplaces 2023 Open Enrollment Report” CMS.gov, 2023 ⤶
- “Health Insurance Marketplaces 2023 Open Enrollment Report” CMS.gov, 2023 ⤶
- ”HEALTH INSURANCE MARKETPLACES 2024 OPEN ENROLLMENT REPORT” CMS.gov, 2024 ⤶

